KEYWORDS
Leptospirosis, meningitis, tropical disease, zoonosis
INTRODUCTION
Leptospirosis (infection with Leptospira spp) is a widespread zoonotic disease. Although the majority of the case load is seen in tropical areas,1,2 it also occurs in Europe with a reported incidence of 0.13 per 100,000 individuals.3 Leptospirosis is caused by the transmission of a spirochete of the Leptospira genus through direct contact with infected animals or through indirect contact with a contaminated environment, e.g. fresh water.4 A wide variety of mammalian hosts, both feral and domestic/ semi-domestic, serve as infection reservoirs and can excrete Leptospira spp in the urine.4
Leptospira infection may cause a variety of clinical syndromes. The most severe form is Weil’s disease, which has a high mortality and is characterised by high fever, bleeding, icterus and renal insufficiency.2,5 Leptospiral infection may also present with neurological symptoms, such as meningitis, bilateral facial palsy or opsoclonusmyoclonus syndrome.4,6-8 Many patients with leptospiral infection present with headache, fever and neck stiffness and therefore bacterial, tuberculous or viral meningitis may often be suspected prior to the eventual diagnosis of leptospirosis.9-11 Symptoms of meningitis due to leptospirosis occur with and without cerebrospinal fluid (CSF) abnormalities.12
In the Netherlands, approximately 30-40 cases of leptospirosis are reported per year.11 We reviewed the cases of leptospirosis with suspected meningitis identified in a tertiary referral hospital in the Netherlands and performed a review of the literature on leptospiral meningitis.
MATERIALS AND METHODS
We identified all adult patients (≥ 16 years of age) with confirmed leptospirosis in the Netherlands between January 2011 and December 2014. Cases were defined as patients with a positive serology (microscopic agglutination test (MAT), enzyme-linked immunosorbent assay (ELISA)), positive polymerase chain reaction (PCR) and/or a positive culture for Leptospira species. These tests were performed by the World Health Organisation, Food and Agriculture Organisation of the United Nations, World Organisation for Animal Health, and the National Collaborating Centre for Reference and Research on Leptospirosis (NRL) at KIT Biomedical Research, the Royal Tropical Institute in the Netherlands. NRL confirms approximately 99% of the suspected cases of leptospirosis in the Netherlands, and thus could provide the authors with nationwide epidemiological data for this article.
From this dataset we selected patients with leptospirosis admitted at the Academic Medical Centre, Amsterdam, a tertiary referral hospital in the Netherlands, to study clinical characteristics, treatment and outcome. We analysed whether symptoms consistent with bacterial meningitis (neck stiffness, fever and headache) were associated with CSF abnormalities. All patients with abnormal CSF (defined as CSF white blood cell count > 5/ mm3 , total protein > 0.6 g/l or CSF to blood glucose ratio < 0.6) were considered to have leptospiral meningitis.13 We retrospectively collected clinical characteristics, data on ancillary investigations and outcome. The data were processed anonymously. Oral and written informed consent was obtained from all patients with leptospiral meningitis.
REVIEW OF THE LITERATURE
Subsequently, we performed a literature search for leptospiral meningitis on PubMed, using the search terms “leptospir* AND meningitis”, and ““Neurologic Manifestations”[MeSH] AND leptospir*”. We also searched for cohort studies and reviews about leptospirosis using the search term “leptospir*”. The search was updated until 20 March 2015.
Articles reporting children or animals, duplicate articles and articles in which no specific data were given for leptospiral meningitis patients were excluded. Leptospiral meningeal involvement was defined as a combination of 1) fever with one of the following signs: neck stiffness, altered consciousness or other meningeal signs,12 and 2) detection of Leptospira species in blood and/or CSF by PCR or culture, and/or detection of leptospiral antibodies by serology (MAT and/or ELISA). When CSF was abnormal (see Methods section), the diagnosis of meningitis was established. In an analysis of clinical data we systematically scored baseline and presenting characteristics, clinical course and outcome.
Differences between groups were calculated by means of Fisher’s exact test. Articles with neither an abstract nor access to the full text were excluded. Studies written in English, German, French, Dutch, Spanish, Italian and Portuguese were included.
RESULTS
Between January 2011 and December 2014, 196 cases of leptospiral infection were identified at the NRL in the Netherlands, of which 104 contracted leptospirosis abroad (53%) and 92 contracted leptospirosis in the Netherlands (47%) (figure 1). The mean calculated annual incidence from 2011 to 2014 was 0.30 per 100,000 inhabitants.
Within this period we observed a threefold increased incidence in 2014 (0.57 per 100,000) compared with 2011-2013 (average 0.21 per 100,000). Furthermore, in 2014, leptospirosis was contracted in the Netherlands in 62% of the cases, compared with an average of 33% in 2011-2013.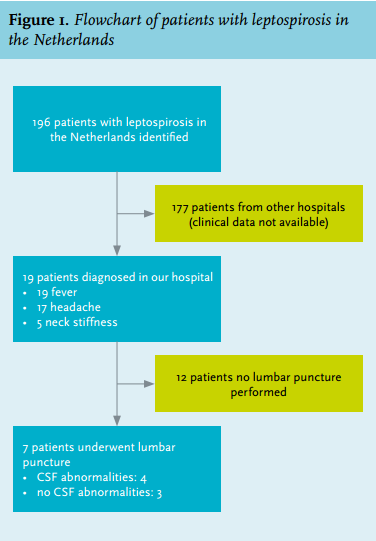
In our hospital, 19 adult cases of leptospirosis (10%) were identified based on a positive serology and/or PCR and/or culture. All 19 patients presented with fever, 17 (89%) presented with headache and five (26%) with neck stiffness. The median age was 27 years (range 17-61 years) and 15 patients were male (79%). Eighteen patients contracted leptospirosis abroad (95%) and one patient contracted leptospirosis in the Netherlands (5%).
In seven patients (37%) there was a clinical suspicion of meningitis, for which a lumbar puncture was performed. Four patients with CSF abnormalities were diagnosed with leptospiral meningitis. Three patients had no CSF abnormalities (figure 1), of which one patient had not been abroad and had not been in contact with animals. The incidence of meningitis in leptospirosis in our hospital was 21% (4 out of 19 patients). The patients with leptospiral meningitis are described below.
Case 1
A 27-year-old Dutch patient was admitted to the hospital in Laos with fever, myalgia, shivers and vomiting. He had been travelling through Vietnam, Laos, Cambodia and Thailand, where he had been swimming. He was treated with antibiotics but no source of infection was found. When he returned to the Netherlands a few days later, he presented with recurrent fever (temperature 38.5°C) and progressive headache. Physical examination showed conjunctivitis and neck stiffness. Laboratory examinations showed the following: creatinine 62 µmol/l, leukocytes 6.4 x 109/l, C-reactive protein (CRP) 3.6 mg/l, serum glutamic oxaloacetic transaminase (SGOT) 23 U/l, serum glutamic pyruvic transaminase (SGPT) 15 U/l, and bilirubin 5 µmol/l. Lumbar puncture showed turbid CSF with 734 leukocytes/ mm3 (75% polymorphonuclear leukocytes), protein level of 0.63 g/l, and CSF to blood glucose ratio of 0.45. The IgM ELISA for leptospirosis was positive. The patient was treated with 1 million IU penicillin intravenously four times a day for seven days. He was discharged in a good clinical condition without sequelae.
Case 2
A 45-year-old Dutch patient presented with fever, headache, nausea and diarrhoea. He had been travelling through Singapore, Thailand and Indonesia two weeks prior to admission, where he had suffered from gastroenteritis after he fell off a boat during rafting and ingested fresh water. Physical examination showed bilateral conjunctivitis but no other abnormalities. Laboratory examination showed the following: erythrocyte sedimentation rate (ESR) 101 mm/h, CRP 106 mg/l, leukocytes 10.8 x 109/l, creatinine 413 µmol/l, SGPT 36 U/l, and bilirubin 8 µmol/l. The Leptospira IgM lateral flow test was positive and patient was treated with oral amoxicillin and discharged. However, the next day, he presented again with aggravated headache. Neurological examination now showed neck stiffness, for which a lumbar puncture was performed. This showed turbid CSF containing 628 leukocytes/mm3 (86% polymorphonuclear leukocytes), protein level of 0.92 g/l and a CSF to blood glucose ratio of 0.41. The IgM ELISA and MAT were both positive, the probable infecting serogroup was Grippotyphosa. The patient was treated with 12 million IU penicillin intravenously daily for three days followed by oral amoxicillin (750 mg three times daily) for one week. He was discharged in a good clinical condition without sequelae.
Case 3
A 20-year-old Dutch patient presented with headache, fever, nausea and diarrhoea. The symptoms appeared a week after returning from a holiday in Borneo, where he had swum in fresh water. Physical examination showed bilateral conjunctivitis and neck stiffness. Laboratory examination showed the following: CRP 45.7 mg/l, leukocytes 6.2 x 109/l, SGOT 354 U/l, SGPT 305 U/l, bilirubin < 2 µmol/l, and creatinine 236 µmol/l. Lumbar puncture showed turbid CSF containing 1200 leukocytes (predominantly lymphocytes, percentage not specified), protein level of 0.89 g/l and a CSF to blood glucose ratio of 0.52. The MAT and IgM ELISA for leptospirosis were positive and showed Leptospira serogroup Australis. The patient was treated with 12 million IU penicillin intravenously for four days followed by oral amoxicillin (750 mg three times daily) for five days. He was discharged in a good clinical condition without sequelae.
Case 4
A 22-year-old Dutch patient presented with fever, headache, cough and nausea. The symptoms appeared a week after returning from a backpack trip in Malaysia, Borneo and Thailand for two months. She had not swum in fresh water, but had slept in rice fields in Thailand. Physical examination showed a temperature of 40.5°C and neck stiffness. Laboratory examination showed the following: leukocytes 12.9 x 109/l, CRP 62.3 mg/l, creatinine 93 µmol/l, SGOT 58 U/l, SGPT 18 U/l, and bilirubin 8 µmol/l. Lumbar puncture showed clear CSF with 11 leukocytes/ mm3 (100% mononuclear cells), a protein level of 0.21 g/l and a CSF to blood glucose ratio of 0.60. The MAT, IgM ELISA and PCR for leptospirosis were positive and showed Leptospira serogroup Mini. Patient was treated with 100 mg doxycycline twice daily for seven days. She was discharged in a good clinical condition without sequelae.
Review of the literature for leptospiral meningitis
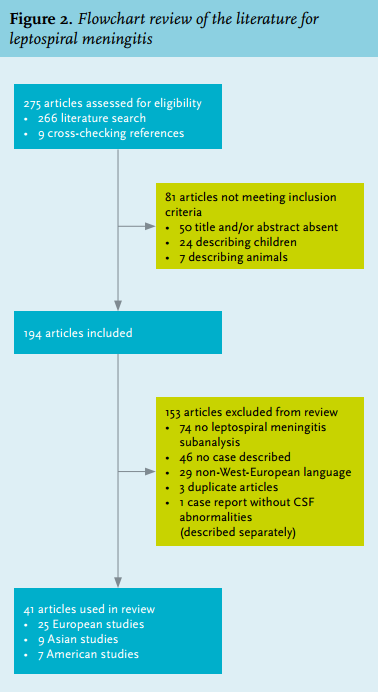
A total of 41 relevant articles published between 1947 and 2014 were identified, describing 366 adults with leptospiral meningitis (figure 2).9,12,14-52 The number of included patients per study varied between one and 162 patients. Studies were performed in Europe (25), Asia (9) and America (7) (figure 2).
The median age of the patients was 33 years (range 17-77 years) and 51 of 62 (82%, 95% CI 72-92%) were male (table 1). Two out of 26 (8%) patients were immunocompromised (95% CI 0-16%). A known aetiology was reported in 32 of 33 patients (97%, 95% CI 91-100%); seven had been in contact with fresh water (five swimming, one fishing, and one window cleaning in an endemic area), six worked with cattle, five had been in contact with dogs, five had been in contact with rats, four were farm workers, two lived in a rural area endemic for leptospirosis, one worked in sewers, one was a horse trainer and one was a hunter. In one patient, no aetiology was found. In an article describing 162 patients with leptospiral meningitis, no aetiology per patient was reported, but the patient group mainly consisted of farmers.47
Headache was reported in 65 of 69 patients (94%, 95% CI 88-100%). Fever was reported in 100 of 102 patients (98%, 95% CI 93-100%), neck stiffness in 77 of 83 (93%, 95% CI 87-99%) and altered consciousness in 8 of 54 patients (15%, 95% CI 5-25%). The classic triad of fever, altered consciousness and neck stiffness53 was present in 5 of 39 patients (13%, 95% CI 3-23%).
The median CSF leukocyte count was 206 leukocytes/mm3 (range 6-2072). All but one of the patients in whom the CSF leukocyte counts were known had a leukocyte count under 2000, with a predominance of lymphocytes (95%, 95% CI 92-98%) in most patients (224 of 236; 95%, 95% CI 92-98%). The CSF protein was known in 39 patients and the CSF glucose in 27 patients. The median CSF glucose was 2.5 mmol/l, while the median CSF protein was 1.10 g/l. In 190 of 208 patients (91%, 95% CI 87-95%), CSF protein was normal, and CSF glucose was normal in 201 of 207 patients (97%, 95% CI 95-99%), while CSF leukocytes were elevated (> 5/mm3 ). In all patients, antibodies to Leptospira were detected by blood serology (either ELISA or MAT); no Leptospira were detected in CSF by culture or PCR.
A total of 245 patients (91%) were treated with antibiotics (mostly penicillin and doxycycline). Twenty-three patients were not treated with antibiotics. One patient was treated with dexamethasone and received antibiotics (penicillin) as well.48 Eight of 229 patients (3%, 95% CI 1-5%) died during hospital admission, of which five had received antibiotics. The cause of death was reported in two cases and consisted of respiratory insufficiency46 and gastrointestinal bleeding.27 The mortality rate in patients who were not treated with antibiotics was 13% compared with 2% in patients treated with antibiotics (Fisher’s exact test, p = 0.04).
Three of 56 patients (5%) had sequelae; one patient was not able to walk until two months after discharge,48 one patient had transient renal insufficiency38 and one patient had neurocognitive defects which resolved after a few weeks.22 Two articles describing two case reports of patients with meningeal symptoms but normal CSF were identified.25,54 When combining these patients and our three patients with meningeal symptoms without CSF abnormalities, we identified five male patients with a median age of 27 years (range 20-47). Two had had animal contact, two travelled to a tropical area and one (one of our patients) worked in the municipal cleansing department. All five presented with headache and fever and two with neck stiffness. Diagnosis was established by blood tests; no leptospiral antibodies or DNA were detected in the CSF. All recovered without neurological sequelae.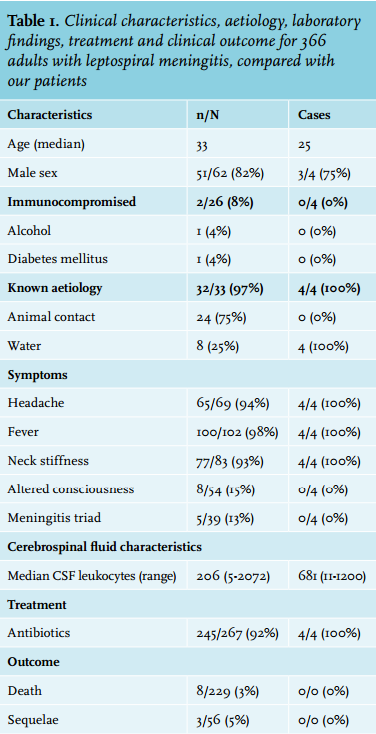
DISCUSSION
We found a low incidence of leptospirosis in the Netherlands: 0.30 per 100,000 inhabitants in the period 2011-2014. In the period 2011-2013, the calculated annual incidence was 0.21 per 100,000 inhabitants, while the annual incidence in Europe in 2010 was 0.13 per 100,000 inhabitants.3 In 2014, however, a threefold increase was observed in the incidence of leptospirosis in the Netherlands: 0.57 per 100,000 inhabitants. The contribution of travelling to leptospirosis in the Netherlands has been up to 50% since 199510,11,55 and was 33% in the period 2011-2013, but in 2014, the majority of patients (62%) contracted leptospirosis in the Netherlands. This increase is currently being investigated (unpublished data).
In our hospital, 18 out of 19 patients and 6 out of 7 patients with suspected meningitis contracted leptospirosis after fresh water contact while travelling in Southeast Asia, which has been reported to be the main risk factor for leptospiral infection worldwide.56 The high contribution of travelling to leptospirosis in our hospital, compared with the national results, is probably caused by most patients being diagnosed at the AMC Department of Tropical and Travel Medicine. Only one patient had not been abroad, but worked at the municipal cleansing department where he could have been infected through contact with sewage water.47
From the 19 patients with leptospirosis identified in our hospital, all had fever (100%), 17 had headache (89%) and 5 had neck stiffness (26%). In general, headache and fever are common symptoms in leptospirosis which have been reported in 60-100%,4 and neck stiffness is found in 10-20% of the cases,10 which confirms our findings.
The incidence of meningitis in leptospirosis is relatively low despite the high frequency of headache and neck stiffness, although there could be an underestimation since not all patients undergo a lumbar puncture. In a cohort study of 63 cases, 12 patients (19%) were diagnosed with leptospiral meningitis,4 which is similar to the incidence of meningitis in leptospirosis in our hospital (21%).
In our review of leptospiral meningitis, headache was seen in 94%, fever in 98% and neck stiffness in 93% of cases. When a patient presents with meningeal symptoms after fresh water contact in tropical regions or direct or indirect contact with animal urine, the diagnosis of leptospiral meningitis should be considered.
Our review showed that most patients with leptospiral meningitis have a mildly elevated CSF leukocyte count and a normal CSF glucose and protein. In a cohort study performed in 2008, CSF pleocytosis was seen ranging from 16 to 850 leukocytes/mm3 . 4 In this cohort study CSF analysis of patients with suspected leptospiral meningitis showed that 50% of patients had CSF pleocytosis,4 which is similar to our case series (4 out of 7, 57%). In most patients in our study, CSF leukocytes mainly consisted of lymphocytes, but two of our cases with leptospiral meningitis had predominantly polymorphonuclear leukocytes in their CSF. This may be due to the timing of the lumbar puncture; polymorphonuclear leukocytes are often predominant early in the clinical course, and later replaced by lymphocytes.16
The necessity of a lumbar puncture in patients with leptospirosis has not been studied. In general, if the diagnosis of leptospirosis has not been confirmed in patients with suspected meningitis, cerebrospinal fluid examination is vital to determine whether the patient has meningitis, and what the cause is. However, in patients with confirmed leptospirosis, cerebrospinal fluid examination does not have additional value since the treatment is similar in patients with and without leptospiral meningitis, unless a second diagnosis is being considered.
In our review, we found a significantly increased mortality in patients not treated with antibiotics compared with those who were treated with antibiotics (13% vs 2%; p = 0.04). However, only a small number of the patients (8%) did not receive antibiotics and the reasons for not treating those patients were unknown. In a recent Cochrane review, there was insufficient evidence for using antibiotics in leptospirosis, but no conclusions for ‘severe leptospirosis’ (not specified) could be drawn.57 No association was established between the different antibiotic treatments ceftriaxone, doxycycline, cefotaxime and penicillin in leptospirosis and outcome. Most patients with leptospiral meningitis are treated with doxycycline or penicillin, which is the currently advised treatment regimen for leptospirosis (doxycycline 100 mg twice a day, or penicillin 1.5 million units four times a day).54,57,58
Our study has several limitations. We did not have clinical information about patients with leptospirosis attending other hospitals in the Netherlands, and therefore our case series is not representative for leptospirosis in the Netherlands. This is reflected in the high proportion of patients in our hospital who contracted leptospirosis abroad (95%) compared with the national average (53%). Furthermore, patients may have contracted leptospirosis and thus have a positive serology, but may have another diseases as well, such as Epstein-Barr viral infection or hepatitis.
For our review, we could not include articles written in non-West-European languages, e.g. Polish and Russian, due to insufficient knowledge of the language. Finally, there could be a publication bias since physicians may not report patients with leptospirosis and meningeal symptoms in whom no CSF abnormalities are found, when CSF culture was negative, or when no lumbar puncture was performed.
In conclusion, leptospirosis in the Netherlands had an annual incidence of 0.30 per 100,000 inhabitants in the period 2011-2014 and was contracted abroad in 53% of the cases. In the case of suspected meningitis and a history of travel to tropical areas or direct/indirect contact with animal urine, tests for leptospirosis should be considered. Leptospirosis commonly presents with headache and fever, but only a proportion of patients have meningitis. Approximately 50% of patients with suspected leptospiral meningitis have CSF pleocytosis and most have a normal CSF glucose and protein. When the diagnosis of leptospiral infection has been confirmed, lumbar puncture does not have clinical consequences, unless there is a differential diagnosis that needs to be considered. Treatment with penicillin or doxycycline usually leads to a favourable outcome.
ACKNOWLEDGEMENTS
The authors thank Hans van der Linden of the Royal Tropical Institute for providing the epidemiological data on leptospirosis in the cases suspected of leptospiral meningitis.
DISCLOSURES
The authors report no conflicts of interests. MCB is supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw; NWO-Veni grant 2012 [916.13.078]). DvdB is supported by grants from the Netherlands Organization for Health Research and Development (ZonMw; NWO-Vidi grant 2010 [016.116.358]), and the European Research Council (ERC Starting Grant 281156). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
REFERENCES