To the Editor,
With interest we read the article by Boon et al. about a 39-year-old female with Guillain-Barré syndrome (GBS) requiring artificial ventilation who developed takotsubo syndrome (TTS) shortly after intubation.1 We have the following comments and concerns.
TTS was not only associated with the eight cases listed in Boon’s article.1 If other terms describing takotsubo syndrome, such as stunned myocardium, stress cardiomyopathy, broken heart syndrome, or reversible (transient) cardiomyopathy, are considered and also atypical types of GBS are included, takotsubo syndrome has been reported in many more cases (table 1). The axonal type of GBS was associated with stunned myocardium in a 27-year-old Chinese female, who recovered under immunosuppression and plasmapheresis.2 TTS was additionally reported in a 59-year-old Indian male with GBS and dysautonomia who recovered under immunomodulating therapy and heart failure treatment within three months.3 A further case of a 82-year-old female with classical GBS was reported from the USA.4 This patient recovered completely under plasma exchange but the cardiac therapy was not mentioned.4 In the case of a 33-year-old Filipino male, TTS was the initial presentation of GBS.5 TTS recovered completely under diuretics exclusively and GBS resolved upon immunoglobulins.5 Possibly, also the case of a 68-year-old female with GBS reported by Goldmann in 2006 describes TTS since myocarditis was only suspected and not confirmed by endomyocardial biopsy.6 Together with Boon’s cases, at least 13 cases of GBS-associated TTS have been reported.
Triggers of TTS are usually fear or pain. Fear may be spontaneous or triggered. Triggered fear may be endogenous (e.g. another illness) or exogenous (e.g. aggression, pain). The authors do not mention any trigger for the TTS. What was the trigger of TTS in the presented case? Was it the stress of respiratory insufficiency and dyspnoea prior to intubation? Was there another fearful event or did she experience severe pain prior to respiratory insufficiency?
Catecholamines Catecholamines are contraindicated in TTS. Why did the patient receive norepinephrine? Was it because of unawareness of the diagnosis? Did the TTS further worsen under this treatment?
Overall, this interesting case adds to the understanding of GBS as a trigger of TTS. Since TTS in GBS may significantly determine the outcome of these patients, it is essential to diagnose TTS instantly by taking chest pain seriously and initiating creatine kinase, troponin, and proBNP determination, ECG recordings, echocardiography and appropriate cardiac treatment. Myocarditis needs to be excluded before diagnosing TTS Whether immunomodulation improves or worsens, the outcome of TTS remains questionable. 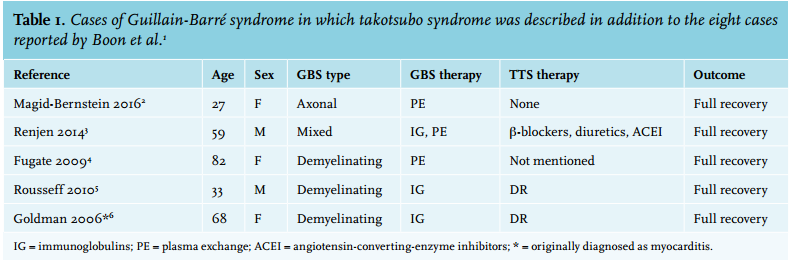
REFERENCES