KEYWORDS
Arthritis, auto-immune, Graves’ disease, methimazole, thiamazole, thionamides
INTRODUCTION
Graves’ disease is the most common cause of hyperthyroidism, occurring predominantly in women and typically between the age of 20 to 50 years. The disease is caused by thyroid-stimulating immunoglobulins, activating the thyrotropin receptor on the follicular cells of the thyroid gland to secrete and synthesise thyroid hormone. Apart from the typical clinical features for any form of thyrotoxicosis (e.g., hyperactivity, tachycardia, weight loss), Graves’ disease may present with distinct signs and symptoms, such as Graves’ ophthalmopathy and, less commonly, dermopathy and acropachy (clubbing). In most parts of the world, the first-line treatment for Graves’ hyperthyroidism is the lowering of thyroid hormone synthesis by thionamides, such as thiamazole (methimazole), carbimazole, or propylthiouracil (PTU). Common side effects of thionamides include rash, urticaria, and arthralgia. Here, we describe a case of a lesser-known side effect of thionamides.
CASE REPORT
A 41-year-old woman was referred to our outpatient clinic for thyrotoxicosis. She reported agitation, hair loss, change in bowel habits, and fatigue. She had no ophthalmologic complaints and there was no history of recent fever or thyroid pain. Her laboratory results showed thyrotoxicosis with positive thyroid-stimulating immunoglobulins (table 1). A thyroid scintigraphy showed homogeneous uptake of technetium-99m, matching the diagnosis of Graves’ disease. We prescribed thiamazole 30 mg once daily and planned to continue with block and replace therapy for the duration of one year.
Twenty days later, the patient contacted us because of pain and swelling in her hands, right knee, and right ankle. She reported having fever (38.5 °C) a few days previously, but her temperature was now normal. Physical examination revealed arthritis with limited movement of the metacarpophalangeal and proximal interphalangeal joints of the 2nd and 3rd fingers on both hands (figure 1). Although painful, the knee and ankle did not evidently show clinical signs of arthritis. Laboratory evaluation showed normal erythrocyte sedimentation rate, C-reactive protein and leucocyte values, and improving free thyroxine levels (table 1). Rheumatoid factor, anti-cyclic citrullinated peptide antibodies, and HLA-B27 were negative. We suspected thiamazole-related arthritis and prescribed naproxen 500 mg two times a day for two weeks, resulting in satisfactory improvement in symptoms to only minor pain in the right knee, without signs of arthritis. After stopping naproxen, she reported minor pain of the hands and right knee for a few weeks, after which the complaints spontaneously disappeared.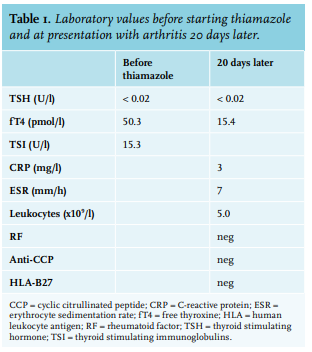

DISCUSSION
Thionamides inhibit the function of thyroid peroxidase, thereby preventing organification of iodine to tyrosine residues and the coupling of iodothyrosines in the thyroid gland. Thionamides can be dosed to completely block thyroid hormone synthesis with addition of levothyroxine substitution therapy (block and replace therapy), or they can be titrated to reduce the amount of thyroid hormone synthesis to satisfactory levels. The most reported side effects of thionamides include rash, urticaria, and arthralgia, mostly well-tolerated and easily treated. Agranulocytosis is a rare but feared complication that can develop abruptly and is a reason to immediately discontinue thionamide-therapy.
Apart from the more common arthralgia, thionamidetreated patients can also present with overt arthritis. The symptoms mostly present as a migratory poly-arthritis, but cases of mono-arthritis or episodic arthritis have also been described.1-3 A classic presentation consisting of myalgia, poly-arthritis, fever, and rash has been termed antithyroid arthritis syndrome.4,5 In an observational study in 500 patients with hyperthyroidism receiving either PTU or thiamazole, rheumatic symptoms were observed in 1.6%, only secondary to skin eruptions (1.8%).4 The symptoms typically present within 2-3 months after initiation of therapy, although arthritis at up to three years has been reported.3,6,7 As most cases did not present with swelling or erythema, the incidence of overt arthritis is expected to be substantially lower, but still abundantly reported in literature.3,8,9 Our patient did report a fever at the onset of pain that spontaneously abated after several days. A rash was not observed. Although causality cannot officially be established in this case study, we have multiple arguments that make a causal relation between thiamazole and arthritis very likely. Both the pattern of poly-arthritis, the fever, and the time-relation with thiamazole matches descriptions in literature.1-7 An alternative diagnosis seems less plausible, as the patient reported no typical symptoms of a viral (e.g., Epstein-Barr virus, hepatitis B or C, parvovirus B19) cause of the arthritis other than the abated fever. In addition, an auto-immune disease is unlikely, given the normal inflammation markers, the good clinical response to NSAIDs and the disappearance of symptoms even after cessation of the NSAID therapy.
Thionamide treatment (especially PTU) has been associated not only with arthritis, but with several auto-immune syndromes, including potentially severe anti-neutrophil cytoplasmic antibodies (ANCA)-associated vasculitis and drug-induced lupus. Apart from musculoskeletal symptoms, cutaneous lesions and fever, these syndromes can present with renal involvement, serositis, or pulmonary involvement, together with positive auto-antibodies such as anti-nuclear antibodies (ANA) and p-ANCA.10-12
The exact mechanism for the development of thionamideinduced auto-immunity is unclear, but several hypotheses have been proposed, such as neutrophil-induced generation of reactive drug metabolites causing auto-immunity in immune compartments;13 binding of the thiol group of thionamides to macromolecules (such as thyroglobulin), inducing auto-immunity by acting as a hapten;8 or disturbed regulation of immune function by incorporation of thionamide metabolites in the DNA.14
Most literature suggests abrupt cessation of the causative drug after diagnosing thionamide-related arthritis to prevent further auto-immune effects. Switching to an alternative thionamide treatment has been successful in some cases,2,15 but high rates of cross-reactivity regarding side effects of antithyroid drugs has been demonstrated.4 Further treatment consists of non-steroidal anti-inflammatory drugs (NSAIDs), usually for one to three weeks. Some authors suggest the use of corticosteroids for more severe or unresolved arthritis, but their efficacy was never established.7,8 Other than recommended in literature, we chose not to withdraw treatment with thiamazole in our patient, as the arthritis was not extensive and the response to NSAID treatment was satisfactory. After withdrawal of naproxen two weeks later, the patient did report continuous minor pain in the hands and knee, without clinical signs of arthritis, and disappearing spontaneously in a few weeks.
CONCLUSION
In conclusion, thionamide-related arthritis is a relatively uncommon side effect of thionamide treatment, usually presenting with migratory poly-arthritis, but expressing large variations in clinical and laboratory features, with rare cases of drug-induced lupus or ANCA-associated vasculitis. Severe presentation warrants acute withdrawal of the causative agent, but our case suggests that milder forms can be successfully treated with anti-inflammatory agents alone. Recognition of the syndrome is essential for timely and effective treatment.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES