KEYWORDS
Copeptin, diagnosis, diabetes insipidus, hypotonic polyuria
INTRODUCTION
Hypotonic (urine osmolality < 800 mOsm/kg, typically < 300 mOsm/kg) polyuria (> 50 ml/kg/24 hours) is a challenging problem in clinical practice;1,2 the differential diagnosis includes central or nephrogenic diabetes insipidus (DI) and primary polydipsia (PP), after excluding causes of solute diuresis (glucose, maltose, urea, sodium, glycine, and mannitol).2 The incidence rate of central diabetes insipidus (CDI) is 3 to 4 per 100,000 population per year and the 5-year prevalence rate is 23 per 100,000 population, with a higher prevalence in children and older adults in a Danish cohort.3 The incidence of X-linked nephrogenic diabetes insipidus (NDI) in the general population of Canadian provinces varied from 8.8 to 58 per million male live births for the period 1988–1997.4 PP is present in 11-20% of chronic psychiatric patients.5 CDI results from the deficiency of the hormone arginine vasopressin (AVP) in the pituitary gland or the hypothalamus.6 The severity of resulting hypotonic polyuria is dependent on the extent of neuro-hypophyseal damage, resulting in either partial (partial CDI) or complete (complete CDI) deficiency of AVP secretion.6 NDI results from inherited or acquired resistance to AVP in the kidneys and can also be partial or complete.7,8 CDI and NDI must be differentiated from PP, which involves excessive intake of large amounts of water despite normal AVP secretion and action.5,9 Contrary to popular belief, history and clinical data may be of limited use because patients with preserved thirst mechanisms do not differ much in their laboratory parameters (see table 1).10,11 The historical gold standard of the indirect water deprivation test to differentiate these disorders has inherent limitations that lead to difficulties with interpretation6 and may lead to misclassification resulting in incongruous treatment and potential harm to the patient. Moving forward, a test with high diagnostic accuracy is required to classify these disorders correctly.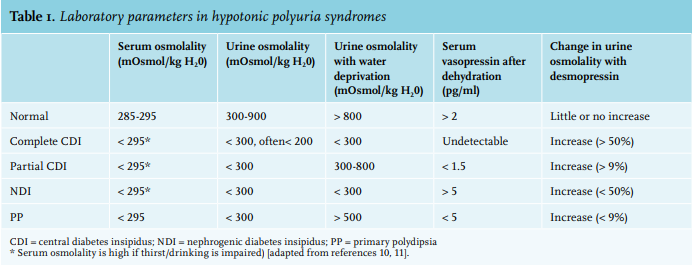
Clinical history and radiology
There is an overlap between the symptoms of DI and PP. Except in the rare condition of adipsic CDI, all three patient groups typically have intact or increased thirst with polyuria and polydipsia.12,13 Traditionally, patients with CDI were thought to have a sudden onset of persistent symptoms, more nocturia, and a preference for cold beverages compared to PP patients.14 However, in a prospective study, more than one-third of DI patients had an insidious onset of symptoms and the majority of those diagnosed with PP preferred cold beverages and had persistent symptoms.1 The unenhanced posterior pituitary magnetic resonance imaging (MRI) was thought to be a useful investigation approach to differentiate between hypotonic polyuria subtypes. The pituitary bright spot is an area of hypersensitivity in the sagittal view on T1-weighted images, which was reported to be absent in patients with CDI in earlier studies.15 There are conflicting case reports of a persistent bright spot in a few patients with CDI.16 Loss of the bright spot has also been seen in congenital NDI, in approximately one-third of patients with PP, and in older adults.1,17,18 Thus, bright spot absence is not a useful test for categorising patients correctly.
Indirect (water deprivation test) and direct AVP measurement
The diagnostic tests for hypotonic polyuria syndromes evolved after the studies on hypophysectomised dogs demonstrated a lack of anti-diuretic response with osmotic stimulation.19 The same concept, inadequacy of urinary concentration, after water deprivation and administration of exogenous arginine vasopressin (AVP), was applied to humans with promising results.20,21 In 1970, Miller et al. described a standardised protocol of indirect water deprivation from their analysis of 36 patients (29 with CDI, 2 with NDI, and 5 with PP) diagnosed clinically and/or by failure to respond to hypertonic saline.10 This test was based on an indirect assessment of AVP activity by measuring urine osmolality following prolonged dehydration, and again after injection of desmopressin. Once dehydration was significant enough to induce thirst, if urine osmolality remained < 300 mOsm/kg and did not increase by > 50% after desmopressin, NDI was diagnosed. Complete CDI was diagnosed if the urine osmolality increased by > 50% after desmopressin injection. In partial CDI and PP, urine concentration increased to 300-800 mOsm/kg, with an increase of 9-50% in partial CDI and < 9% in PP after desmopressin injection. However, there was a wide overlap of urine osmolality amongst the different subgroups. Recent attempts to validate these criteria revealed an overall diagnostic accuracy of only 70% (9 of 9 patients with complete CDI, 16 of 17 patients with partial CDI, 1 of 2 patients with NDI, and 9 of 22 patients with PP).14 The reason for failure of the indirect water deprivation test is multifactorial and includes small patient numbers which were used to establish reference values, weak vasopressin stimulation in some patients secondary to failure to achieve a hyperosmolar serum, and renal pathophysiology. Chronic polyuria can cause washout of the renal medullary concentration gradient and downregulate aquaporin-2 (AQP2) channels resulting in loss of urinary concentration ability in CDI and PP.22-24 However, AVP-V2 receptors may be up-regulated in chronic partial CDI, increasing anti-diuretic response to low levels of AVP.25,26 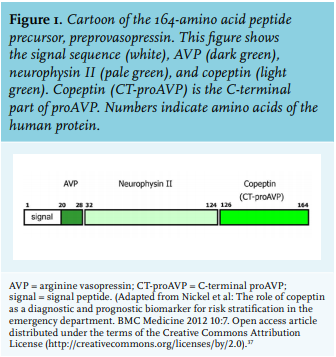
The result of these opposing mechanisms is a convergence of distinct underlying disorders to a near-identical urinary phenotype. Moreover, in NDI there may be only partial resistance to AVP and clinical resemblance to partial CDI.27,28 Thus, it becomes difficult to differentiate amongst these conditions exclusively based on the water deprivation test. In a seminal paper, both direct AVP measurements after osmotic stimulation and standard indirect water deprivation test correctly identified severe CDI, but discrepant results were seen in patients with PP.29 Of the 10 patients who appeared to have PP by the indirect test, three had unequivocal evidence of AVP deficiency by direct measurement. This was further corroborated by a uniformly excellent response to desmopressin therapy. In another study of 50 patients with polyuria-polydipsia syndrome, direct AVP measurements showed a dismal diagnostic accuracy of around 38% (2 of 9 patients with complete CDI, 5 of 17 patients with partial CDI, 16 of 22 patients with PP, and neither of 2 patients with NDI were diagnosed correctly). The authors concluded that plasma AVP levels were not reliable for distinguishing PP and CDI, particularly the partial form of CDI.12 The problems of high pre-analytical instability of commercial AVP assays, lack of a comparative diagnostic gold standard, and paucity of a defined normal AVP response to osmolality makes AVP measurements a non-reliable test in current clinical practice.30-32
Copeptin: biochemistry, physiology, and measurement
Copeptin, first discovered in 1972 from the posterior pituitary of pigs, originates from the precursor pre-provasopressin with AVP and neurophysin II (figure 1).33-37 It is a 39 amino acid glycosylated peptide with a leucine-rich core that is thought to modulate the three-dimensional unfolding of vasopressin into a functioning molecule.38 AVP measurement is technically difficult due to AVP instability, high in vitro thermolability, and a short half-life of 10-44 minutes; copeptin has a half-life of approximately 86 minutes, high ex vivo stability, and is easy to measure. Copeptin is stable in EDTA plasma and serum for seven days at room temperature and 14 days at 4 0C, allowing for delayed analysis.36 Reliable results are available rapidly from a small volume of plasma or serum (50 µl) using either a manual sandwich immunoluminometric assay (LIA) or a less complicated commercially available automated immunofluorescent (KRYPTOR) test for a reasonable price, without the need for pre-analytical laboratory processes.39-41
The stimuli for copeptin mimic those for AVP with similar release kinetics in response to changes in osmotic pressure (correlation coefficient 0.94) and low arterial blood volume/pressure.42-44 Given the equimolar 1:1 ratio between the two peptides, copeptin can serve as a surrogate for AVP.36,43 The plasma copeptin concentration in health ranges from 1.0-13.8 pmol/l (median: 4.2 pmol/l) in adults36 and 2.4-8.6 pmol/l (mean 5.2 ±1.56 pmol/l) in children.45 Renal clearance is responsible for partial elimination of copeptin but is not the main determinant of its concentration.46,47 Females tend to have lower values, but median values are comparable across age groups.36,48 Increase in copeptin levels has been observed during fasting, post-exercise, and psychological stress, while levels significantly decreased after small amounts of water ingestion.43,49-51 Variability was not observed in response to the menstrual cycle but there does appear to be a minor impact of circadian rhythm in some patients.52,53 Copeptin has also been studied as a biomarker for various stress states like ischemic stroke, septic shock, traumatic brain injury, lower respiratory tract infections, and myocardial infarction.36,39
Copeptin: an evidence-based journey in the differentiation of hypotonic polyuria subtypes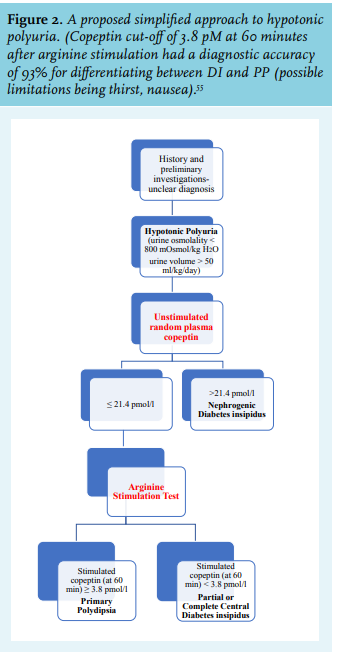
Over the last decade, copeptin has replaced plasma vasopressin due to its stability and is now an important test in hypotonic polyuria work up. In a pioneering prospective study of50 patients with hypotonic polyuria and 20 healthy subjects, plasma AVP and copeptin levels were measured after a standard water deprivation test.14 In case of discrepancy between direct and indirect test results, reference diagnosis was established based on medical history, clinical findings, and therapeutic response to desmopressin. The osmotically-stimulated copeptin was found to have an overall diagnostic accuracy of 83%. Baseline copeptin values greater than 20 pmol/l identified patients with NDI, and concentrations below 2.6 pmol/l indicated complete CDI. The ratio of copeptin increase during an 8-hour dehydration period to the serum sodium concentration measured after 16 hours of water deprivation increased the diagnostic yield to 94% (sensitivity 86% and specificity 100%) in discerning patients with PP from partial CDI. The major limitation of this study and with others is the relatively small patient numbers and lack of a true gold standard test with which the copeptin results could have been compared.
A prospective multicentre observational cohort study of 55 patients with the history of polyuria and polydipsia evaluated the accuracy of copeptin.54 A standardised combined water deprivation and a 3% saline infusion test were performed. Water deprivation started at 08.00 hours (h) as long as plasma sodium did not exceed 147 mmol/l and continued until the plasma sodium surpassed that value. Once plasma sodium was greater than 147 mmol/l, if urine osmolality was less than 300 mmol/l, desmopressin was given. If plasma sodium did not exceed 147 mmol/l by 13.00 h, hypertonic saline was administered. A single baseline copeptin level > 21.4 pmol/l (without prior fluid restriction) differentiated NDI from other aetiologies with a 100% sensitivity and specificity, rendering water deprivation unnecessary in these patients. An osmoticallystimulated copeptin ≥ 4.9 pmol/l (at sodium levels > 147 mmol/l) differentiated between patients with PP and patients with partial CDI with sensitivity and specificity of 94%. The specificity further improved to 96% when complete CDI patients were included in the analysis. AVP measurements performed poorly for differentiation between partial CDI and PP yielding a definite diagnosis of PP in only 44% of patients with this entity.
In a landmark multicentric study of 156 hypotonic polyuria patients, both indirect water deprivation and hypertonic saline infusion tests were performed on separate days.1 In the latter test, plasma copeptin was measured when the plasma sodium level had increased to at least 150 mmol/l. In the absence of a gold standard, the diagnosis was determined at study completion by two endocrinologists based on available history and laboratory data without knowledge of the copeptin levels. The overall diagnostic accuracy in distinguishing patients with PP from CDI with hypertonic saline infusion test was 96.5% (sensitivity 93%, specificity 100%) with a predefined copeptin level of > 4.9 pmol/l compared to 76.5% (sensitivity 86.4%, specificity 69.5%) with the indirect water deprivation test. Increasing the predefined copeptin level to > 6.5 pmol/l increased sensitivity further without compromising specificity. The hypertonic saline infusion test was also more accurate in correctly distinguishing PP from partial CDI, compared to the indirect water-deprivation test (p < 0.001). Adding water deprivation plasma copeptin ratios did not improve the diagnostic accuracy of the indirect water deprivation test in distinguishing PP from CDI, as had been demonstrated in a previous study. The proposed morning copeptin level of < 2.6 pmol/l after an overnight water deprivation to identify patients with complete CDI had a diagnostic accuracy of only 78%. All three patients with NDI had a copeptin level of > 21.4 pmol/l. The investigators concluded that hypertonic saline-stimulated copeptin measurement was superior to the indirect water deprivation test in distinguishing CDI from PP. However, the hypertonic saline infusion was associated with more side effects and required close monitoring of sodium levels to achieve an increase in plasma sodium concentration within the hyperosmotic range followed by a rapid reversal to a safe value.
For this reason, arginine infusion, which is known to stimulate the release of anterior pituitary hormones, was explored as an easier and safer way to stimulate copeptin without inducing hypernatraemia. The copeptin response to arginine was compared with the final diagnosis for hypotonic polyuria based on the results of indirect water deprivation test, patient characteristics, and treatment response in prospective study design.55 Patients with NDI identified based on a single baseline copeptin value (as defined by previous studies) were excluded from the study protocol. The arginine stimulation test (arginine infusion over 30 minutes) was assessed in development and validation cohorts of patients with CDI (21 in the development cohort, 19 in the validation cohort) or PP (31 in the development cohort, 27 in the validation cohort). The comparator cohort included 50 healthy adults (20 in the development cohort, 30 in the validation cohort) and 42 children (who had suspected growth hormone deficiency) in the development cohort. Arginine infusion increased copeptin concentrations 2.2 times in patients with PP, 1.2 times in the patients with CDI, and 1.5-1.8 times in the healthy control cohort. In the pooled dataset, an argininestimulated copeptin cut-off of 3.8 pmol/l measured at 60 minutes was associated with a diagnostic accuracy of 93% (sensitivity 93% and specificity 92%) and 90% (sensitivity 93% and specificity 88%) in differentiating between CDI and PP, and between partial CDI and PP, respectively. Moreover, the copeptin response was not associated with other clinical and biochemical variables in their post-hoc analysis.
Post-hoc head-to-head comparison of 60 patients (23 with DI, 37 with PP) between arginine-stimulated vs hypertonic saline-stimulated copeptin response revealed their diagnostic accuracies as 93% and 100%, respectively, in distinguishing between patients with DI and PP. However, the arginine-stimulated protocol had fewer adverse effects (less than 5%) with arginine stimulation (including two participants with vomiting who were not included in the main dataset) compared to > 70% with hypertonic saline) with a significantly lower test burden. This short, practical, and relatively safe arginine-stimulated copeptin response could become the new standard test for the workup of hypotonic polyuria when the diagnosis is unclear from initial history and laboratory investigations (figure 2). The results of the CARGOx study when available (use of copeptin measurement after arginine infusion for the differential diagnosis of diabetes insipidus, NCT03572166) will be helpful in this regard.
CONCLUSION
The differential diagnosis of hypotonic polyuria is challenging, especially distinguishing partial DI from PP. The current diagnostic standard of the indirect water deprivation test has several limitations, including a long test duration and poor diagnostic accuracy especially in distinguishing partial DI and PP. Over the past decade, copeptin has emerged as a biomarker for various disorders. Plasma copeptin levels are highly correlated with AVP; high baseline values correctly identify patients with NDI. For differentiating PP from CDI, hypertonic saline stimulated copeptin level of > 4.9 pmol/l had a higher diagnostic accuracy than the water deprivation test. The arginine-stimulated copeptin response circumvents the shortcomings of the hypertonic saline test (longer test duration, more side effects) and provides a novel, pragmatic, and safe work-up approach to diagnose hypotonic polyuria syndromes.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES