KEYWORDS
Cushing’s disease, hair cortisol analysis, pituitary apoplexy
INTRODUCTION
Pituitary apoplexy is an infrequent but life-threatening complication of pituitary adenomas.1 Haemorrhage in the pituitary gland causes immediate mass effects, resulting in severe headaches sometimes accompanied by visual field compromise and hypopituitarism. When apoplexy occurs in a hormonally active adenoma, this might induce spontaneous remission of the clinical syndrome. Rarely, pituitary apoplexy is the presenting symptom of a functioning pituitary adenoma. In these cases, clinical suspicion of Cushing’s disease or acromegaly might arise at presentation. Due to spontaneous remission of active hormone production, it is not possible to biochemically confirm this diagnosis in retrospect.2-7 Resolution of clinical symptoms during follow up retrospectively suggests the diagnosis. However, we describe a patient with Cushing’s disease presenting with pituitary apoplexy, who was biochemically in remission at presentation. By using hair cortisol analysis, we were able to confirm the clinical suspicion of Cushing’s disease, thereby enabling us to adequately anticipate remission of Cushing’s disease.
CASE REPORT
A 31-year-old woman was referred to our outpatient clinic. She had been admitted to a foreign hospital with thunderclap headache. Additional magnetic resonance imaging (MRI) showed pituitary apoplexy in a pituitary macro adenoma, which had not been diagnosed before (figure 1). At the time of presentation, she had complaints of light-headedness, loss of appetite, and nausea with vomiting. Her medical history reported hypertension, type 2 diabetes mellitus, polycystic ovary syndrome, and hypothyroidism, all diagnosed within a timeframe of three years. She had not been using any steroid medication. Physical examination was suggestive for Cushing’s syndrome, i.e., moon face, acne, facial hirsutism, central obesity, and quadriceps atrophy. Further physical examination was unremarkable. Laboratory testing was consistent with complete anterior hypopituitarism: cortisol 09:00 hr < 28 nmol/l (normal 240-700 nmol/l); thyroid stimulating hormone (TSH) 3.3 mE/l (normal 0.4-4.0 mE/l); free T4 (FT4; thyroxine) 6 pmol/l (normal 10-22 pmol/l); lutenizing hormone (LH) 2E/l; follicle stimulating hormone (FSH) 4E/l; and estradiol < 44 pmol/l. There was no visual impairment due to optic nerve compression, and therefore, no indication for acute pituitary surgery. Hydrocortisone therapy of 80 mg a day was started to treat the secondary adrenal insufficiency. 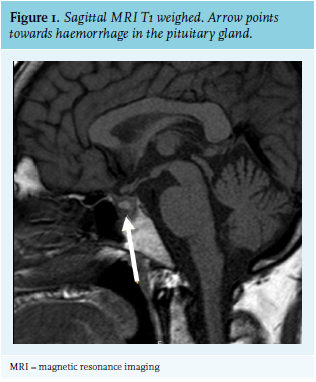
Gradually, all deficiencies were adequately treated. Due to the presence of complete anterior hypopituitarism at presentation, the clinical suspicion of pre-existing Cushing’s disease could not e biochemically confirmed. However, hair cortisol analysis was performed on her 22 cm long hair. The results showed cyclic but significantly and consistently elevated cortisol levels for the last 22 months: average 25 pg/ml (reference value in normal controls 2.7 pg/mg hair, 95% CI 0.7-10.5 pg/mg hair).8 We therefore confirmed the diagnosis of Cushing’s disease in our patient cured by pituitary apoplexy. After establishing the diagnosis, we were able to taper corticosteroid therapy at a rate that is indicated for Cushing’s disease in remission to prevent steroid withdrawal symptoms. Additionally, anticipating remission of hypertension and type 2 diabetes, the antihypertensive and glucose-lowering medication could be reduced.
DISCUSSION
Spontaneous curation of Cushing’s disease by pituitary apoplexy is infrequent and difficult to prove. Hair cortisol analysis can be used to prove the diagnosis in retrospect. Pituitary apoplexy is a rare endocrine emergency resulting from bleeding or infarction in the pituitary gland often resulting in acute loss of pituitary function. It occurs in about 4.8-5.8% of pituitary macro adenomas and mostly it involves non-functioning adenomas.9,10 Pituitary apoplexy is the first presenting symptom of a pituitary tumour in 7.3% of all cases.10 Remission of Cushing’s disease by pituitary apoplexy is an infrequent event given that pituitary apoplexy mostly occurs in non-functioning adenoma. A similar course of disease with spontaneous remission of Cushing’s disease after symptomatic pituitary apoplexy has been described in several case reports. In previously described cases, the diagnosis of Cushing’s disease was based on histology after surgery, or on the clinical course of resolution of symptoms of Cushing’s disease after apoplexy.1
This is the first case in which the diagnosis was proven in retrospect by hair cortisol analysis. Hair cortisol analysis is a relatively new diagnostic tool which is not yet widely used. It is currently being studied for clinical applications.11,12 To date, it has been studied in the setting of diagnosing cyclic Cushing’s disease, overtreatment with steroid therapy in adrenal insufficiency, as marker of adverse cardiologic risk profile, and in the setting of several psychiatric disorders.11,13 It is a retrospective test in which cortisol levels in 1 cm of hair represents the average serum cortisol level during the period of one month. The process of hair cortisol analysis is extensively described in the article of G. Noppe et al, 2015.8 The hair is cut from the posterior vertex and divided into small portions. Then the steroids are extracted and measured using liquid chromatography mass spectrometry/mass spectrometry (LC-MS/MS). The sensitivity and specificity are remarkably high compared to other tests for Cushing’s disease. The reported sensitivity and specificity using immunoassay hair cortisol analysis are respectively 93% and 90%.11
Although hypocortisolism was identified in the blood samples at initial presentation, this was not reflected in the hair cortisol measurements. In our patient, the average hair cortisol level was, although cyclic, persistently far above the upper limit of normal in the past 22 months as can be seen in figure 2, retrospectively proving that our patient was suffering from a previously unidentified Cushing’s disease. Figure 2 shows a decrease in cortisol level starting from the moment of the pituitary apoplexy (between one and two months prior to the hair sample). These measurements represent average cortisol levels during a period of one month, and in this case, the average of temporary hypocortisolism and relative hypercortisolism due to initial supraphysiologic dosage of hydrocortisone. By proving spontaneous remission of Cushing’s disease using hair cortisol analysis, it is possible to adequately treat patients with initial high dose of steroid for prevention of steroid withdrawal. Additionally, one can anticipate remission of diabetes and hypertension. Therefore, hair cortisol analysis provides a useful tool for the clinician to provide proper care. In our opinion, hair cortisol analysis should be considered in patients presenting with pituitary apoplexy and signs or symptoms of Cushing’s disease.
In conclusion, we present a case of a previously unidentified Cushing’s disease, spontaneously in remission after pituitary apoplexy. This is the first case that is proven in retrospect by hair cortisol analysis.
PREVIOUS PRESENTATIONS
Previously presented at the Dutch Internist Days (Nederlandse Internisten Dagen) 2018 – MEC Maastricht
DISCLOSURES
The authors declare no conflicts of interest. EFCvR is funded by a Vidi grant from the Netherlands Organization of Scientific Research NWO (grant number: 91716453). No further funding or financial support was received.
REFERENCES