KEYWORDS
Chemotherapy dose modification, chemotherapy-induced neutropenia, febrile neutropenia, lipegfilgrastim, real-world evidence
INTRODUCTION
Occurrence of neutropenia is a well-known risk of chemotherapy (CT), and in particular, severe and febrile neutropenia (FN) can significantly impact the outcome of cancer treatment, resulting in an increase in infectionassociated morbidity and mortality.1 Moreover, neutropenic events may lead to changes in the treatment plan, such as dose reductions and/or delays in subsequent cycles or even switching to less effective treatment options, ultimately decreasing overall response and life expectancy.1,2 To reduce the risk of CT-induced neutropenia, preventive treatment is required and granulocyte-colony stimulating factors (G-CSFs) have been recognised as effective therapies3 as they stimulate neutrophil production and differentiation.4 In a meta-analysis of randomised clinical trials, administration of G-CSFs as primary prophylaxis (PP) was shown to also reduce all-cause mortality compared with patients not receiving G-CSFs, with the decrease in risk varying with CT dose and schedule.5 Current European guidelines recommend G-CSFs support for all patients receiving a CT regimen associated with a high (> 20%) or intermediate (10–20%) risk of FN, for dose-dense or dose-intense CT strategies, or in subsequent CT cycles following a FN episode. Recentlyidentified factors such as older age (≥ 65 years) or low neutrophil count should also be included in an assessment of risk carried out before each cycle.6 Real-world data on the routine use of G-CSFs prophylaxis for CT-induced neutropenia and FN are now available from the United States, where an increase in the use of G-CSFs from 2010 to 2016 led to a decrease in the incidence of FN among cancer patients at intermediate and high risk in the first cycle of CT, despite a clear underutilisation of the recommended prophylaxis.7
Lipegfilgrastim (Teva Pharmaceutical Industries Ltd, Israel), a glycopegylated G-CSF, has previously been shown to reduce the duration of neutropenia and incidence of FN in adult cancer patients treated with cytotoxic CT8-11 and was approved for use in the European Union in July 2013.12 In a large prospective, non-interventional study conducted in several European countries, the effectiveness and safety of lipegfilgrastim as PP or secondary prophylaxis (SP) in real-world settings was evaluated in adult patients with different tumour types receiving cytotoxic CT.13,14 Here we report data on treatment delays and modifications and incidence of neutropenic events in cancer patients in the Netherlands who received lipegfilgrastim in routine clinical settings.
METHODS
Study design and participants
This phase 4, prospective, observational study was conducted in eight centres in the Netherlands between October 2015 and August 2017. Male and female patients who received cytotoxic CT with or without biological/ targeted therapy (BT) for solid and haematological malignant cancer in real-world settings were eligible for enrolment in the study. Lipegfilgrastim was administered as prescribed by the treating physician and according to medical indication, independent of the intention to include the patient into the study. Inclusion criteria were age ≥ 18 years and administration of lipegfilgrastim as PP or SP (following a neutropenic event in a previous CT cycle) of CT-induced neutropenia. Patients were excluded from study enrolment if they had chronic myeloid leukaemia and myelodysplastic syndromes, were pregnant or lactating women, or if they received investigational products as part of a clinical trial.
The study was conducted in full accordance with the Helsinki Declaration and the guidelines for Good Clinical Practice, Good Epidemiological Practice, Good Pharmacoepidemiology Practices, and Good Pharmacovigilance Practices and was approved by institutional ethics committees at each site. All patients signed an informed consent form prior to enrolment in the study.
Patients were followed from the first use of lipegfilgrastim until 6-8 weeks after the last dose. Data pertaining to patient demographics and baseline characteristics, FN risk factors, CT/BT data (dose delay, reduction, omission), incidence of FN or neutropenia, FN-related hospitalisation and use of anti-infectives and antimycotics, and safety were recorded on electronic case report forms. In agreement with the European Society for Medical Oncology (ESMO) guidelines, FN was defined as an oral temperature of > 38.3°C or two consecutive readings of > 38.0°C for two hours and an absolute neutrophil count of < 0.5 × 109/l, or expected to fall below 0.5 × 109/l.15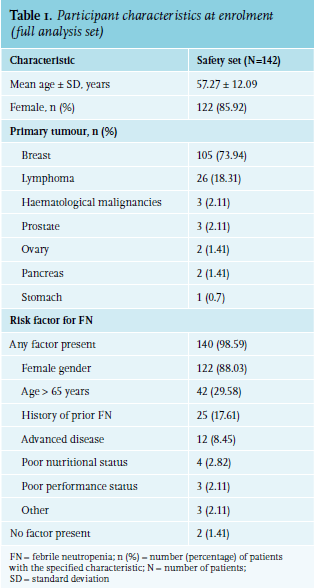
Study objectives
The primary objective of the study was to describe the effect of lipegfilgrastim used in prophylaxis on CT dose modifications, including delay, omissions, and reduction of CT dose administration, in patients receiving cytotoxic CT for solid and haematological cancers, according to routine clinical practice in the Netherlands. Secondary objectives included the description of cancer patients treated prophylactically with lipegfilgrastim in terms of tumour type and stage, CT setting, demographic characteristics, comorbidities and FN risk, and assessment of safety.
Safety assessments
Adverse events (AEs) and serious AEs (SAEs) were coded with the Medical Dictionary for Regulatory Affairs version 20.0 and summarised by preferred term. All AEs were classified by severity as grade 1 (mild), 2 (moderate), 3 (severe or medically significant), 4 (life-threatening, urgent intervention needed), and 5 (fatal), according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.16 The relationship of AEs to lipegfilgrastim administration (not related/related) was assessed by the investigators.
Statistical analyses
A sample size of 150 participants was estimated based on feasibility considerations in the entire European population. Analyses were carried out on the full analysis set, which included all enrolled patients meeting eligibility criteria. Patients were stratified by subgroups, as follows: type of prophylaxis (PP versus SP), tumour type, tumour stage, CT regimen use (adjuvant vs metastatic), gender, age, Eastern Cooperative Oncology Group (ECOG) performance status, and FN risk (low, intermediate, and high). No imputation of missing values was performed. Analyses were mainly descriptive and interpreted in an explorative way.
RESULTS
Patient characteristics
In total, 144 patients were enrolled in the study and 142 were evaluated (two patients did not receive lipegfilgrastim during the study period). All 142 patients received at least one dose of lipegfilgrastim followed by a post-cycle efficacy evaluation. The patients’ baseline characteristics are presented in table 1. The mean age was 57 years, with 49 (34.51%) patients being aged ≥ 65 years (table 1). Most patients (94.37%) were Caucasian and the large majority (85.92%) were women. Lipegfilgrastim was received as PP for 106 (74.65%) patients and as SP for 36 (25.35%) in 596 cycles (there were a total of 613 cycles for the entire study population). Lipegfilgrastim was administered as SP due to the occurrence of FN (for 15 patients) or neutropenia (in 30 patients), with most patients starting to receive lipegfilgrastim as SP in the second (10, 7.04%) or third (15, 10.56%) CT cycle.
Forty-nine (34.51%) patients were classified as low risk, 37 (26.06%) as intermediate risk, and 56 (39.44%) as high risk of FN. The most frequent individual risk factors for FN were female gender (122 patients, 88.03%) and age > 65 years (42 patients, 29.56%) (table 1). Two participants (1.4%) had liver disease and 8 (5.6%) had cardiovascular disease.
CT was planned for all patients, with most participants receiving it in the adjuvant (79 patients,55.63%) and neo-adjuvant (51 patients, 35.92%) setting. Eight patients (5.63%) received CT in a metastatic setting, 2 (1.41%) patients as maintenance, and 2 (1.41%) as other setting. For 28 patients (19.72%), BT was also planned. Most patients received docetaxel/doxorubicin/ cyclophosphamide (37 patients, 26.06%), doxorubicin/ cyclophosphamide (37 patients, 26.06%), or doxorubicin/ cyclophosphamide/vincristine with or without prednisone (17 patients, 11.97%) as CT treatment.
Chemotherapy dose modifications
Overall, 607 administered cycles were analysed, and the delay of CT ranged between 0 and 3.5 days, with a mean delay of 0.8 ± 3.34 days. The mean delay period was higher in patients using lipegfilgrastim as SP than as PP (1.17 versus 0.71 days) and in patients aged ≥ 65 years compared with those aged < 65 years (table 2). Overall, delays were recorded for 37 (26.06%) patients, with higher proportion of patients reporting delays in SP versus PP, blood tumour versus breast tumour, and intermediate/low risk versus high risk of FN subgroups (table 2).
Dose reductions were recorded for 3 (2.11%) female patients with breast cancer using lipegfilgrastim as PP (one reduction each in cycle 1, 2, and 4). All three had an Eastern Cooperative Oncology Group (ECOG) status < 2 and a low risk of FN. No CT dose omissions occurred. No dose reduction of BT treatment was reported in any patient. Only one BT treatment omission was recorded, for a male patient aged ≥ 65 years, receiving lipegfilgrastim as PP; the patient had lymphoma, used CT in the adjuvant setting, and presented intermediate risk of FN.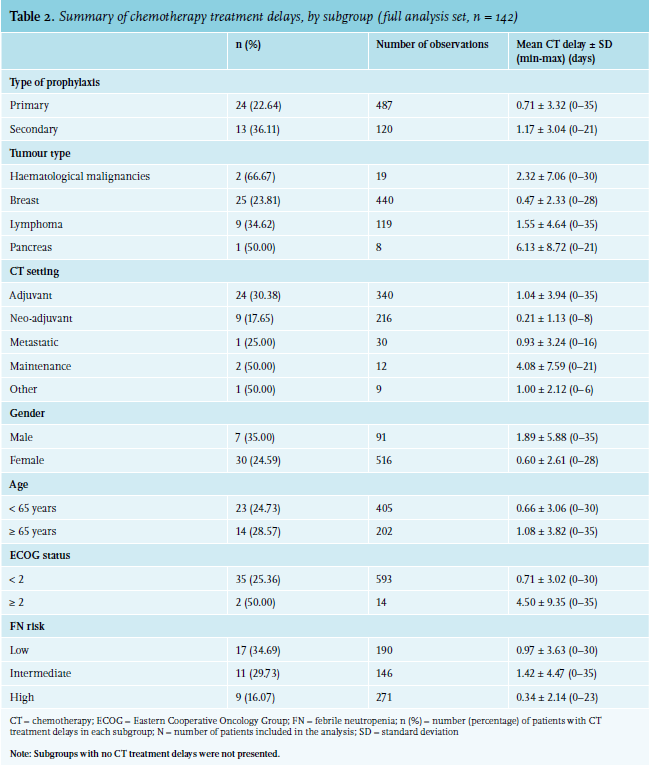
Incidence of neutropenia and hospitalisation/treatment
Overall, 8 (5.63%) patients reported FN. The majority (six) were female with an ECOG score < 2 and three received lipegfilgrastim as PP. FN was reported in four patients with lymphoma, two with breast cancer, one with pancreatic cancer, and one with stomach cancer. Most participants with reported FN used adjuvant CT (five patients) and were at low (three patients) or intermediate (four patients) risk of FN. Grade III/IV neutropenia at a given time were recorded in 14 (9.86%) patients, with 9 (6.34%) and 5 (3.52%) patients reporting grade III and grade IV neutropenia, respectively. Four (2.82%) patients were hospitalised due to FN, 2 (1.41%) due to CT-induced neutropenia; 39 (27.46%) patients were hospitalised for other reasons, not related to neutropenic events. Anti-infective treatment was used in 54 (38.03%) patients, with a mean duration of 13.97 ± 16.84 days. For 5 (3.52%) and 1 (0.70%) of these patients, the use was related to FN and CT-induced neutropenia, respectively (Supplementary material, table S1)*. Five (3.52%) patients were administered intravenous anti-infectives for FN. Antimycotic treatment was used a total of 49 times in 23 (16.31%) patients (Supplementary material, table S2)* and the mean duration was 27.41 ± 28.72 days; the treatment was not related to FN and CT-induced neutropenia for any of the patients.
Safety
At least one treatment-emergent AE (TEAE) occurred in all patients, the most frequently reported being myalgia (22.53%), bone pain (17.61%), pyrexia (14.79%), and back pain (11.27%). Most TEAEs (88.66%) were mild or moderate in nature and 41.06% were considered related to study medication. Myalgia (19.01%), bone pain (16.20%), back pain (7.75%), and arthralgia (5.63%) were the most frequent TEAEs related to lipegfilgrastim administration. Three patients (2%) discontinued lipegfilgrastim prematurely due to adverse events. Overall, 55 SAEs were recorded in 30 (21.13%) patients, with the most frequent being pyrexia and pneumonia (each in seven cases), and FN and lung infection (each in four cases); most of them were mild to moderate. In total, 14 SAEs in 10 (7.04%) patients were considered as possibly related to lipegfilgrastim administration. Fatal events were reported for 2 (1.41%) patients, with the AEs leading to death being advanced disease and cancer progression for one patient and ureteral stent infection (urosepsis) for the other. Neither deaths were considered related to lipegfilgrastim.
DISCUSSION
This is the first study assessing CT dose modifications following administration of lipegfilgrastim as prophylaxis for CT-induced neutropenic events in real-world settings in Dutch patients. Our findings confirm effectiveness and raises no new concerns about safety when compared to clinical trial results. This study showed that dose delay was the most common modification of CT treatment following lipegfilgrastim administration, occurring in 26.06% of patients, while CT dose reductions were rare, reported for only 2.11% of patients. No CT dose omissions occurred. Dose delays were reported more frequently in patients receiving lipegfilgrastim as SP than those receiving it as PP (36.11% versus 22.64%).
In the real-world prospective study assessing the same objectives in a larger, European population which included Dutch patients, slightly lower rates were observed for overall dose delays, reductions, and omissions, but similar to our study, dose modifications were reported with higher frequency, when lipegfilgrastim was used for SP rather than for PP (for 28.1% and 20.1% of patients).14 In contrast to our observations, dose modifications in Belgian patients occurred in 33.3% and 52.4% of patients receiving lipegfilgrastim as PP and SP, respectively, with dose reductions being more common. Of note, most Belgian patients had breast cancer and more than half (54.7%) received dose-dense regimens, unlike in our study.17 In another non-interventional study conducted in 2489 German patients undergoing CT in routine clinical practice (NADIR), dose delays were observed at lower rates than in the current study for 11.2% of patients.18 However, in the NADIR study, 16.3% of patients received lipegfilgrastim as SP, compared to 25.35% of the Dutch population, which may constitute one of the possible explanations for the difference in dose delay rates. In contrast, dose reductions were reported more frequently in the NADIR study in 19.6% of patients.18 However, these comparisons are hindered by differences in the characteristics of patients in each study, which varied, also in terms of tumour type, stage, metastasis, age, performance status, or FN risk. Of note, a higher percentage of Dutch patients were considered at low risk of FN (34.51%), compared with < 10% in the NADIR study.18 In clinical trial settings, the rates of dose delays ranged from 16.2%19 to 30.7%8 of patients in the first cycle after initial administration of lipegfilgrastim, while no dose omissions/reductions were reported, suggesting that dose modifications can vary greatly with demographics, tumour type, and prescribed CT.
Overall, FN was observed in 5.63% of patients in our study and grade III and IV neutropenia occurred in 6.34% and 3.52% of patients. Compared to our study, a lower incidence (2.7%) was observed in the NADIR study for FN and higher rates of severe neutropenia (26.8%) were reported.18 Despite differences in the proportion of patients at low risk of FN and lipegfilgrastim prophylactic administration for the two populations, both studies show that lipegfilgrastim is effective in reducing CT-induced neutropenic events and further confirm effectiveness data observed in phase III clinical trials.8,9,19 Randomised head-to-head trials have been conducted between lipegfilgrastim and pegfilgrastim. A meta-analysis concludes lipegfilgrastim showed a lower, nonsignificant risk of febrile neutropenia compared with pegfilgrastim (risk ratio (RR)=0.34, 95% CI: 0.05, 2.14). Lipegfilgrastim has a statistically significantly shorter absolute neutrophil count recovery time without significant differences in bone pain.20 Moreover, in the current study, the rates of FN/neutropenia-related hospitalisations, intensive care unit stays, and use of anti-infectives/antimycotics were low, suggesting that the associated cost can be decreased considerably when lipegfilgrastim is used as prophylactic treatment of CT-induced neutropenic events. According to several modelling studies, lipegfilgrastim was estimated to be a likely cost-effective alternative to other G-CSFs in patients with breast cancer.21,22
Lipegfilgrastim was well tolerated, with a safety data comparable to that observed in the NADIR study. A comparable proportion of Dutch and German patients experienced SAEs (21.13% versus 18.0%, respectively), and none of the fatal events occurring during the two studies were related to lipegfilgrastim administration.18 Myalgia, bone pain, and back pain were the most frequent lipegfilgrastim-related TEAEs in the current study, consistent with observations from real-life studies and the safety profile assessed in pivotal clinical trials.12,18 Of note, in the NADIR study, patients evaluated the administration as easy to handle and the most frequently documented reason for discontinuing lipegfilgrastim prematurely was that prophylaxis with lipegfilgrastim was no longer considered necessary.18
Our study has several potential limitations. Specific reasons for changes in CT treatment were not collected and therefore, we cannot conclude on a potential association between lipegfilgrastim administration and CT treatment modifications. Analyses were mainly descriptive and the sample size was relatively low, although patients from eight centres in the Netherlands were enrolled in the study which is likely to ensure a representative sample. Selection bias and confounding by indication are potential biases, but the majority of the included patients were at risk of FN (table 1) and lipegfilgrastim support was according to current guidelines.5,6 Data in the entire European population will soon be available and will provide an improved interpretation of the results for the Dutch patients in the larger context of clinical practice in Europe. In conclusion, the use of lipegfilgrastim as either PP or SP during cytotoxic CT treatment led to a relatively low proportion of patients with CT dose modifications or with neutropenic events, in real-world settings in the Netherlands. Administration of lipegfilgrastim was well tolerated, with no new safety concerns arising during the study.
ACKNOWLEDGEMENTS
The authors are grateful to the patients and all hospital staff involved in the study. The authors also thank Petronela M. Petrar (Modis) for medical writing and publication coordination services.
DISCLOSURES
The authors report no conflicts of interest. This work was supported by Teva Pharmaceuticals. All costs associated with the development and publication of the manuscript were covered by Teva Nederland BV.
*Supplementary materials are available from the authors upon request
REFERENCES