KEYWORDS
Emergency department, frailty, geriatric screening method, VMS
INTRODUCTION
Life expectancy and the prevalence of frailty in the Netherlands are increasing.1 Up to 25% of emergency department (ED) presentations are patients aged 65 years or older.2 These patients are at risk of adverse outcomes after discharge, such as readmission, functional decline, and mortality.2 After discharge from the ED, 24% of patients are readmitted in the first three months and 44% in the first six months.3 The average 90-day mortality of these patients is about 10%.3-5 Identifying patients at high risk of adverse outcomes such as death and readmission provides opportunities for preventive geriatric intervention. Frailty is a predictor of adverse medical outcomes in older patients. Frailty is defined as a dynamic syndrome characterised by decreased reserves and resistance to stressors, due to a decline in multiple physiological systems.6 A comprehensive assessment of frailty is difficult to measure in the ED.7 The increasing number of older patients in the ED and prevalence of frailty require the development of frailty screening instruments in the ED. Screening for frailty in the ED is feasible and can improve patient outcomes.8-9
To identify frail patients, many screening instruments are available both worldwide7,10 and in the Netherlands.11 Studies have been conducted investigating diagnostic accuracy of older adult vulnerability screening instruments, but there is a lack of pragmatic, accurate, and reliable tools.7 An instrument that may be used for identifying frail older patients at risk for negative outcomes in older patients presenting to the ED is the Veiligheidsmanagementsysteem ‘VMS’ (Dutch Safety Management Program) for frail older patients.12 This instrument is part of a national program to prevent avoidable injury or death. The complete screener is presented in figure 1. 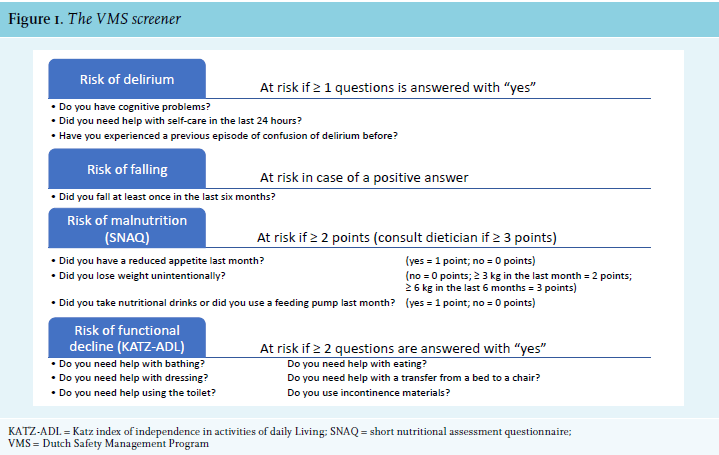
Screening can be performed by a nurse, geriatrician, or physician’s assistant and takes about 4-5 minutes; it identifies patients (aged 70 years or older) at risk for delirium, falls, malnutrition, and functional impairment, who require preventive measures.12,13 In the Netherlands, all hospitalised patients aged 70 years or older are screened but screening is not routinely performed in the ED. The VMS instrument has been shown to be a good predictor for adverse outcomes in older hospital patients.14,15 No previous studies have been done to test the predictive value for patient outcomes of the VMS screener in the ED. This study investigated if the VMS screener identifies patients aged 70 years or older at risk for adverse outcomes (i.e., mortality, functional decline, falls, readmission to the hospital or ED, or a change in living situation) in the ED.
METHODS
This prospective cohort study was approved by the medical ethical committee of the Amsterdam Medical Centre, the Netherlands (registration number W17_209) and the institutional review board at Gelre Hospitals, Apeldoorn and Zutphen, the Netherlands. It was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from all eligible patients before inclusion in the study. The inclusion period ran from May 2017 until August 2017. Because the effect size was unknown, a power analysis was not feasible. The authors aimed to recruit a convenience sample of 200 patients. Patients aged 70 years or older were recruited at the ED of Gelre Hospital Apeldoorn presenting for the following specialties: internal medicine, geriatric medicine, general surgery (including trauma), orthopaedic surgery, gastroenterology, pulmonary medicine, and urology. Gelre Hospital Apeldoorn is a level 2 trauma centre in an urban setting. Inclusion hours were between 10:00 AM and 7:00 PM during week days. Exclusion criteria were: logistical impossibility to include patient (i.e., patient missed for inclusion, unstable medical condition), language barrier (patient not proficient in Dutch or English), severe cognitive impairment (diagnosed by physician at ED or as mentioned in patient records) with no proxy present, no permission to approach the patient by their attending nurse or physician. Age, sex, and specialty for which the patient had been referred was documented for patients for which no informed consent was obtained. All measurements were performed within approximately 30 minutes of presentation at the ED. The following baseline data were collected: age, sex, specialty for which the patient had been referred, living situation (at home, in a residential care facility, in a nursing home), diagnosis of dementia (as stated in medical records), number of different medications, use of a walking device, and whether the reason for the ED visit had been a fall.
VMS screening was performed for all included patients by author HS who had received training by a professional geriatrician. The VMS screener consists of four domains (figure 1): risk of functional decline, risk of falling, risk of delirium, and risk of malnourishment.13 Functional decline was measured using the KATZ activities of daily living (KATZ-ADL) score.16 The SNAQ score is a validated screening instrument for detecting malnutrition.17 Risk of delirium was assessed by asking if the patient had cognitive problems, needed help with self-care in the previous 24 hours, or had experienced a previous episode of delirium. In cases with a positive answer to either of these questions, the risk of delirium was considered present. The risk of falling was assessed by asking if the patient had experienced a fall in the previous six months and considered present in cases with a positive answer.
Patients with incomplete VMS data were excluded from further analysis. The VMS score was calculated by adding up all positive domains, resulting in a score ranging from zero to four. All domains were given equal weight. Domains were not analysed individually because the VMS is already implemented in all Dutch hospitals as a four-domain tool and this will not change. Additionally, in order to divide patients into ‘frail’ and ‘non-frail’ groups, VMS scores were dichotomised using a cut-off point of two or more positive domains, based on previous studies.15,18,19
Treating physicians in the ED were blinded for VMS scores. The primary outcome of this study was 90-day mortality, which was determined by consulting the municipal civil registry. After a follow-up period of 90 days after presentation at the ED, all surviving patients were contacted by telephone to determine secondary outcomes. Three attempts on three different dates at different times were made to contact the patient. If the patient could not be reached after the third attempt, the patient was considered lost to follow up. Secondary outcomes were functional decline, defined as a one-or-more point loss of KATZ-ADL, having experienced a fall during follow up, change in living situation, or a hospital or ED readmission during follow up. A change in living situation was defined as moving to a facility with a higher level of care than before presentation at the ED (e.g., from living on their own to a residential care facility). A composite outcome was created, defined as either death or functional decline (loss of points on KATZ-ADL) at follow up, assuming that patients who had died had also inherently experienced functional decline. This decline could not be quantified by the KATZ-ADL, because the patient must be alive at follow up to determine this score.
Differences between frail and non-frail patients were analysed with the chi-squared test for categorical data. Normality was tested for continuous variables including VMS score with the Shapiro-Wilks test. All continuous variables were not normally distributed at the p < 0.001 level and thus, A Mann-Whitney u test was performed. Positive predictive value (PPV) and negative predictive value (NPV) was calculated for VMS frailty and each outcome. VMS scores were analysed as a continuous variable using ROC curve analysis for each outcome. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., 2017, Armonk, NY). The level of statistical significance was set at 0.05 for all analyses. No funding was received for this study. This paper was written in accordance with the STrenghtening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines.20
RESULTS
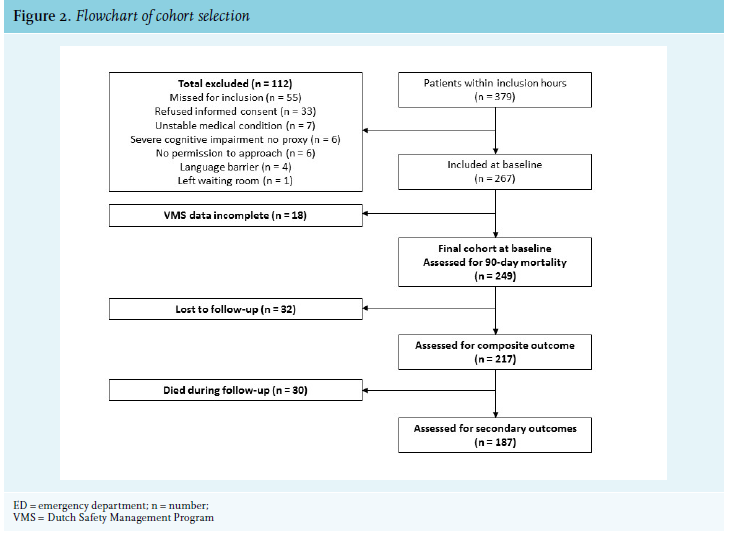
During the study period, 1203 eligible patients presented to the ED, 379 of whom presented within inclusion hours. A total of 112 patients were excluded. Due to a software error in data registration, 18 subjects had to be excluded because their VMS data was incomplete. After 90 days, 30 patients had died. Of the surviving patients, 32 individuals could not be reached by telephone. Cohort selection is summarised in figure 2. Baseline characteristics are shown in table 1.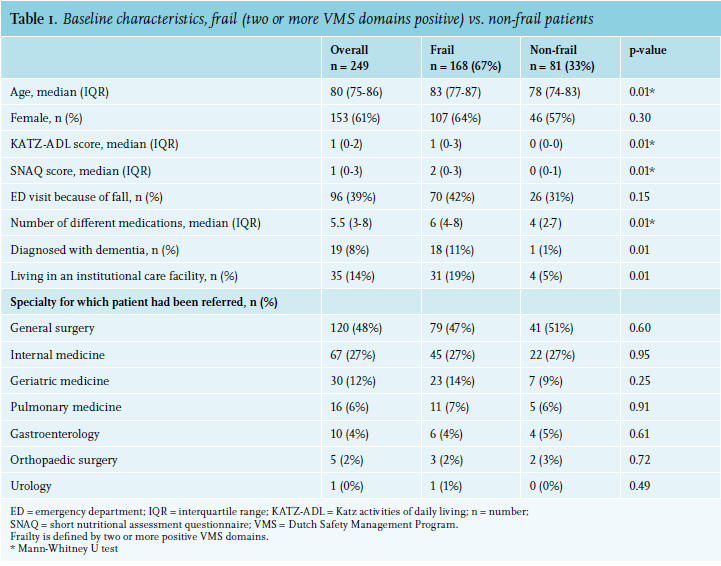
The median VMS score was 2 (IQR 1-3) and 168 (68%) of patients were classified as frail. The median age was 80 years (IQR 75-86) and there were 153 (61%) female patients. Median KATZ-ADL score was 1 (IQR 0-2). Patients were mainly referred to the ED for general surgery, internal medicine, and geriatric medicine.
Frail patients were older [median 83, IQR (77-87)] vs. non-frail patients [median 78 (74-83)], p < 0.01. They were dependent on more activities of daily living, had a higher SNAQ score, and used more medication at baseline. The prevalence of dementia was higher in the frail cohort (n = 18; 11%) vs. non-frail (n = 1; 1%; p = 0.01) and frail patients more often lived in an institutional care facility (frail, n = 31; 19% vs. non-frail, n = 4; 5%; p < 0.01).
The results of all ROC curve analyses are summarised in table 2. The ROC curve analysis for VMS score in relation to 90-day mortality had an area under the curve (AUC) of 0.65, with a 95% CI of (0.54-0.76) and a p-value of < 0.01. A higher VMS score was also associated with a fall during follow up, with an AUC of 0.67 and a 95% CI of (0.56-0.78), p = < 0.01. There was no association between a higher VMS score and the composite outcome (functional decline and death), functional decline (KATZ-ADL), readmission to the ED, readmission to the hospital, or change in living situation during follow up.
The associations between VMS frailty and different outcomes is presented in table 3. Patients classified as frail were more likely to die during follow up in this study: frail, n = 25 (15%) vs. non-frail, n = 5 (6%), p = 0.05 with a PPV 0.15 and an NPV 0.94. They were also more likely to experience a fall after their visit to the ED: frail, n = 27 (22%) vs. non-frail, n = 5 (8%), p = 0.02, with a PPV 0.22 and an NPV 0.92. There was no association between VMS frailty and KATZ-ADL functional decline (p = 0.83), the composite outcome of functional decline and death (p = 0.13), readmission to the ED (p = 0.18) or the hospital (p = 0.81), or a change in living situation (p = 0.94).
DISCUSSION
In this study, frail patients as identified by the VMS admitted to the ED were more likely to die during 90-day follow up or experience a fall, compared to non-frail patients. ROC curve analysis showed that a higher VMS score was also predictive of mortality and of a fall during follow up. The overall predictive value of the VMS screener for adverse outcomes was low.
No previous studies have investigated VMS score in the ED in relation to adverse medical outcomes in the ED. Previous studies investigating VMS score in relation to adverse outcomes target patients who are already hospitalised18,21 or target specific patient populations such as cancer patients22 or orthogeriatric patients.15 These cohorts are not comparable to the cohort presented in this study. The 12% mortality in this study corresponds with previous studies, in which 90-day mortality was between 9% and 12% in older patients presenting to the ED.3
The ED may provide physicians with an opportunity to screen patients in an early stage and implement geriatric interventions, if necessary. There is currently no gold standard to identify frail patients in the ED.23 The VMS screener can provide physicians with useful information regarding deficits in the four different domains, but predictive performance as a screener for adverse medical outcomes seems limited. Total VMS score ROC curve had an AUC < 0.7, which represents poor test performance in predicting outcomes.24 The low positive predictive value of the VMS frailty score means that in practice, some patients would be classified as frail, while not at higher risk for adverse outcomes. The high negative predictive value indicates that the screener can be used to identify patients not at risk for adverse medical outcomes. The ideal screening tool identifies is non-invasive and has a high sensitivity. The VMS meets these criteria and could be a useful first step to determine which patients should undergo additional screening (e.g., comprehensive geriatric assessment). The VMS screener identified 68% of all patients as frail, and it is unlikely that resources are available to provide all these patients with a thorough geriatric follow up. A two-step approach could be considered, using the VMS screening with a high negative predictive value as a first step (i.e., rule-out model), and a second step where patients are screened by a consulting geriatrician by using clinical impression or by using a frailty tool with a high positive predictive value. The patient burden in the ED in the Netherlands is increasing, and screening methods should be both effective and time-efficient. Alternative screening methods, such as the acutely presenting older patient (acuut presenterende oudere patient, APOP) with a PPV of 0.20-0.30 for 90-day mortality and the identification of seniors at risk (ISAR) could also be considered.25,26 However, these screeners only give a total score and do not provide information in specific domains. There are three distinct advantages of VMS screening: 1) It can be performed by any nurse, physician’s assistant, or physician at presentation at the ED or anywhere in the hospital; 2) it is non-invasive and takes only about 2-3 minutes to complete; and 3) the screener identifies four different domains for which non-invasive geriatric measures can be taken immediately, such as fall prevention and delirium prevention. 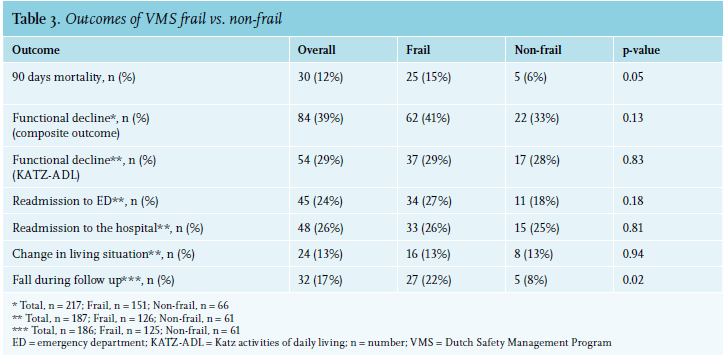
This study has a few limitations. First, due to limited logistical resources, inclusion hours were between 10:00 AM and 7:00 PM on workdays. This resulted in a smaller sample size and the possibility of selection bias. There was no significant difference in mortality between patients included in the final cohort (12%) and excluded patients, including those presenting outside inclusion hours (10%), p = 0.48. Patients who had been referred to the departments of geriatric or internal medicine were more often excluded. It is possible that these patients were more ill and refused to participate in the study. Second, it is possible that patients with a higher VMS score received different treatment then patients with a lower VMS score. Although treating physicians were blinded for VMS score, factors such as comorbidity and older age may have guided decision making, which may introduce bias. Third, external validity of this study may be limited as it was a single centre study and patients presenting to the departments of cardiology and neurology were excluded. To our knowledge, this is the first study to investigate the use of the VMS screener in relation to adverse medical outcomes in the ED. No previous studies have investigated VMS score as a continuous outcome in relation to outcomes in the ED. An important strength of this study was the use of many different important patient outcomes during follow up, such as functional decline and change of living situation. Another strength was that functional decline was determined in two different ways to reduce survival bias. KATZ-ADL is frequently used in follow-up studies to measure a degree of functional decline or functional outcomes.23,25 The authors advise caution regarding this approach for two reasons. First, KATZ-ADL follow-up can only be obtained for patients who are alive after the follow-up period. This holds true for any functional outcome measure and is especially challenging when investigating functional decline in older patients. Second, patients who are not ADL dependent can more easily lose points in KATZ-ADL than patients who are fully dependent on others at baseline. This means that one-point loss of KATZ-ADL does not represent an equal loss of function among patients. Patient-reported outcome measures such as the patient-reported outcome measurement information system for physical function (PROMIS-PF) may be more accurate and patient-centred outcomes and should be used in future investigations.27
In conclusion, the predictive performance of the VMS screener in relation to several important patient outcomes in the ED was studied. Using a cut-off point of two or more positive domains predicts 90-day mortality (PPV 0.15, NPV 0.94) and falls (PPV 0.22, NPV 0.92), but none of the other outcomes. The low PPV shows that many patients classified as frail do not experience adverse outcomes, making the screener less suitable to identify high risk patients. The screener can still be used to get a quick impression of the functional and nutritional and cognitive status of a patient, which can help guide decision making. The high negative predictive value indicates that the screener can identify patients not at risk for adverse medical outcomes, which could be a useful first step to determine which patients should undergo additional screening by comprehensive geriatric assessment.
ACKNOWLEDGEMENTS
Compliance with ethical standards
This prospective cohort study was approved by the medical ethical committee of the Amsterdam Medical Centre, the Netherlands and the institutional review board at Gelre Hospitals, Apeldoorn and Zutphen, the Netherlands. It was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES