CASE REPORT
A 38-year-old male presented at the Emergency Department with non-bloody diarrhoea and acute abdominal pain for one day. Medical history comprised mild chronic obstructed pulmonary disease and daily use of cannabis and amphetamines.
Physical examination showed a severely ill, disorientated, and euphoric patient. He had a respiratory rate of 32 breaths/minute, an oxygen saturation of 98% with 3 litres of supplemental oxygen, a heart rate of 125 beats/minute, a blood pressure of 138/98 mmHg and a temperature of 36.6 °C. There was no nuchal rigidity. We observed blue coloured lips, diffuse petechiae, purpura, and ecchymosis of the extremities, as well as a small healing wound on the right thumb.
Laboratory investigation showed a haemoglobin concentration of 9.8 mmol/l, leucocyte count of 26.0 x 109/l, severe thrombocytopenia with a platelet count of 7 x 109/l, D-dimer 21 mg/l, C-reactive protein 452 mg/l, lactate 8.4 mmol/l, creatinine 248 µmol/l, and urea 13.3 mmol/l. Chest X-ray and computed topography scan of the abdomen did not show abnormalities.
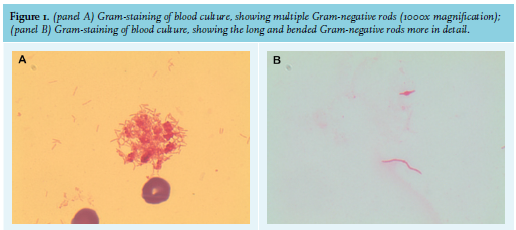
He was admitted to the Intensive Care Unit (ICU) with suspected circulatory shock and supported with fluid administration, norepinephrine, and nitroglycerin. During his ICU stay, the haemoglobin concentration decreased to 3.6 mmol/l due to haemolysis (fragmentocytes present in small numbers, direct Coombs test negative, complement C3 and C4 normal). Differential diagnostic considerations were septic shock with diffuse intravasal coagulation (DIC), thrombotic thrombocytopenic purpura (TTP), (Shiga toxin-mediated) haemolytic uremic sydrome (HUS), and (drug-induced) thrombotic microangiopathy (TMA). We commenced treatment with ceftriaxone, ciprofloxacin, gentamicin, and plasmapheresis. On the third day, both aerobic blood cultures bottles showed growth of long bended Gram-negative rods (figure 1).
WHAT IS YOUR DIAGNOSIS?
See page 215 for the answer to this photo quiz.