KEY WORDS
Implementation, intensive care, point-of-care ultrasound, training program
HIGHLIGHTS
INTRODUCTION
Today, point-of-care ultrasound (POCUS) is considered an important tool for intensivists.1 Reviews and guidelines on POCUS are published but there is still debate surrounding it, including definitions, content, and training requirements,2-8 but POCUS is still considered an indispensable tool for every intensivist.8,9 Although recognised as an important skill by national societies, POCUS is trained differently in various countries.10 In the Netherlands, the Dutch Society for Intensive Care (NVIC) provides a basic course (two days on heart and lungs) and a consolidation course in which 40 supervised heart/lung ultrasound exams are included. In addition to intensivists, the Dutch Society of Internal Medicine recently decided that residents in internal medicine should also be trained in POCUS; a national training program is under construction with some aspects already published.11 While literature provides professionals with theoretical guidelines on how to use POCUS, there is far less literature discussing the practical issues of implementing and training in POCUS. The Rijnstate Hospital Department of Intensive Care has used POCUS since 2009 and in 2017, implemented a training program for residents in internal medicine prior to their intensive care rotation. In this narrative review, we share our experiences with the process of implementing POCUS and how we designed our resident POCUS training program on the basis of current literature. We have received questions from colleagues from other hospitals on these issues and hope that by publishing our experiences, both successes and weakness, we can inform and help other educators who want to develop their own local educational POCUS program.
1. IMPLEMENTING POCUS
This section is divided into three elements: the start, equipment, and collaboration.
1.a. The start
With the increase in publications on the use of POCUS in intensive care, the intensivists of the Rijnstate Hospital Intensive Care Department decided in 2009 that they also wanted to use this technique. Within a week of this decision, the process of POCUS training and implementation was initiated, and training in the basics of cardiac and lung POCUS were provided by an Australian team of POCUS experts (Marek Nalos et al, Nepean Hospital, Australia), a week prior to an international ICU congress. This training-on-the-job approach led to a leap in knowledge and ability to perform basic cardiac and lung ultrasounds by all members of the intensive care staff. Three out of 10 intensive care staff members added skills for abdominal ultrasound by attending a basic abdominal ultrasound in Dusseldorf Germany (Matthias Hofer; http:// medidak.de/semester/sono) and during daily practice, all staff members and residents were trained in using ultrasound during insertion of central venous catheters. As of the writing of this manuscript, the entire intensive care staff is trained in at least basic cardiac and lung POCUS. Two of the staff members are more experienced and participate in national training programs for POCUS for the Dutch Intensive Care and Internal Medicine Societies In our experience, the simultaneous training of the entire staff helped boost POCUS use in our department and we would recommend this approach.

Success: Every intensivist in our intensive care department is trained in basic lung and cardiac POCUS. All procedures, such as the insertion of central lines are guided by the real-time use of ultrasound. We published our view on POCUS content,12,13 and have integrated POCUS into our daily practice. Today, ultrasound is part of daily care at the Rijnstate Intensive Care Department. In almost all patients, thoracic ultrasound is performed during or shortly after admission and if indicated, also abdominal ultrasound (for example, of the kidneys in cases of urosepsis). Ultrasound is also performed in cases of clinical deterioration. POCUS exam results can be described in our electronic health record (figures 1, 2, 3, and 4, in Dutch). We are involved in scientific ultrasound research projects, both self-instigated14,15 and in collaboration with other institutes,16 and are currently investigating the use of POCUS for our emergency team; other projects are in preparation. 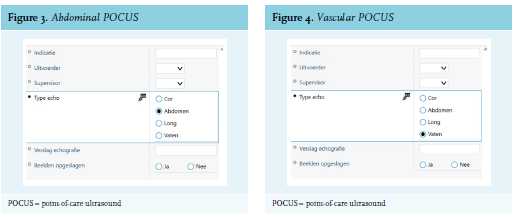
Weakness: The acquisition and retention of POCUS skills took almost a decade and still, not every intensivist in our department has the same POCUS skills. Reasons for the time needed: some have more interest in POCUS than others and POCUS skills must be learned without a pause in daily routine and night shifts. The development of these skills on our ward is not very different from what the literature reports. Although POCUS is seen as an important tool, it is not used on every patient,17 and there are intensive care colleagues who state that an intensivist can still be a good intensivist in the absence of POCUS skills.18
How can we speed up this process? First, by training internal medicine residents, the use of POCUS in the intensive care department will be stimulated. Forty-four percent of Dutch intensivists have internal medicine as their primary specialism (data from NVIC, personal correspondence), meaning that in the near future, these intensivists will already be trained in basic POCUS. A basic ultrasound course is also advised to residents in anaesthesiology but is not obligatory (https://www.anesthesiologie.nl/uploads/ files/Opleiding_LOP2019NVA.pdf); 40% of Dutch intensivists have anaesthesiology as their primary specialism (data from NVIC, personal correspondence). At this moment, there is no national obligatory ultrasound training program for intensive care fellows (https://nvic.nl/sites/nvic.nl), although most fellows will come across POCUS during their fellowship and will be trained on the job. We speculate that in the near future, the Dutch board for intensive care training (GIC) will present formal ultrasound training requirements for fellows which will speed up POCUS implementation in the Netherlands.
In the meantime, current intensive care staff should be motivated to enrol in at least a basic POCUS course. The NVIC basic course is always fully booked, but there are other (inter)national courses (www.deus.nl, https:// www.esicm.org/education/courses-2/lives-mc-basic-courseechocardiography/). Publications like our paper can help generate awareness of POCUS and can stimulate colleagues to start a POCUS implementation process on their own intensive care departments.
It is a challenge to train all intensivists, fellows, and residents in POCUS, and unfortunately, there are too few available educators to train the large number of physicians. Although guidelines exist on the requirements for the POCUS learner on how to achieve competence, there are less-clear guidelines for the requirements of POCUS-educating staff. POCUS trainers can be physicians from different disciplines, preferably certified in echocardiography, but should at least have significant experience in critical care ultrasound.6 In our situation, we combine the knowledge of experienced intensivists (without formal advanced certification) with the knowledge of cardiology and radiology colleagues, who are co-authors of this paper.
Some larger intensive care departments may have one or more cardiologists on staff. According to most guidelines, a fully trained cardiologist can be seen as an advanced ultrasound user, thereby capable of educating others in basic cardiac ultrasound. For intensive care departments without a cardiologist, close cooperation with the local cardiology department is advised.19 An alternative way of ensuring advanced skills is to have one or more intensive care staff members follow an advanced cardiac ultrasound course, for example, the European Diploma in advanced critical Echocardiology (EDEC, https://www.esicm.org/education/ edec-2/), but this requires a significant time investment. To our knowledge, there is no advanced abdominal ultrasound course for intensivists, meaning that for expert help, local radiology departments should be available.
1.b. Equipment
In our opinion, every intensive care department should have their own ultrasound equipment. Today, even the handheld machines are capable of producing adequate images and the development of portable ultrasound systems has contributed to the increased use of POCUS,20 but one should be aware of their shortcomings.21 In this article, we will not discuss the various options; we chose to obtain two high-end ultrasound machines (Philips Affinity) for optimal image quality. In particular, in the beginning when trying to acquire reasonable ultrasound images, it is wise to use an ultrasound machine with optimal image resolution. A hand-held ultrasound device (Philips Lumify) is attached to our emergency trolley and can be used during medical emergency calls in the hospital.
In addition to data storage on the ultrasound machine itself, we encourage the use of digital image storage facilities to be able to re-assess ultrasound examination for quality or educational purposes.
Success: Both our two intensive care wards have their own high-end ultrasound machines and are connected by WIFI to a digital storage facility.
Weakness: We became highly dependent on our ultrasound machines and, in the beginning, had some technical challenges that were resolved together with the Department of Technical Engineering. We advise having a spare machine available in case of break-down or maintenance.
1.c. Collaboration
From the start, we involved the radiology and cardiology departments in our plans. We have previously reported on POCUS as an important tool for intensive care and that this development was embraced by not only international intensive care societies but also by cardiology societies as well.3-5,22,23 We asked the departments of radiology and cardiology to assist us in our ambitions by helping us train our staff, and later our residents, and to share their ultrasound experience and skills. Their involvement enables them to actively contribute to our training program, and by training together, we emphasise the difficulty of ultrasound and the need to be critical towards the acquired ultrasound skills.24 In many cases, the radiology or cardiology departments currently receive much more precise clinical questions from the Intensive Care Department because the POCUS examination is performed upfront. In addition, POCUS is likely to become more widespread and thus, we have an opportunity to shape an effective training program; this view is shared3,4 by scientific cardiology ultrasound societies. The storage of POCUS examinations is encouraged in order to be able to evaluate POCUS examinations afterwards.
During the start of POCUS training, we also collaborated with the pulmonology department, even though they too, were beginners at ultrasound. We still do ultrasound projects together, and recently the Departments of Pulmonology, Radiology, and Intensive Care published a handbook for pulmonary ultrasound (Springer Healthcare Benelux ISBN/ISSN 9789492467225, July 22, 2019, Echografie van de thorax, Corien Veenstra, Michiel Blans et al).
Success: We were fortunate that our cardiology and radiology colleagues were willing to help. Since we were able to discuss our plans in advance, we could take advantage of their advice and consider justified concerns. We were aware of the absolute prerequisite that we had to implement ultrasound in a safe and responsible way. After many years of (inter)national experience with POCUS in the Intensive Care Department, we hope that, in the Netherlands, the controversy on this topic will disappear and we encourage intensive colleagues to discuss POCUS with their cardiology and radiology colleagues. We acknowledge the differences between a POCUS study performed by one of our intensivists, compared with a fully comprehensive ‘normal’ ultrasound study completed by our cardiology or radiology departments, and we have discussed this with both departments prior to developing our program. POCUS is aimed at detecting a limited number of acute clinical problems and its results are immediately useful. This method of using ultrasound is different from the comprehensive ultrasound studies done by cardiologists, radiologists, or their ultrasound technicians. Usually, the latter ultrasound studies are not aimed at a specific clinical situation, but are more often done by examining the heart or all abdominal organs using a fixed framework, with the results given afterwards. Major intensive care and ultrasound scientific organisations state that POCUS can be performed by intensivists, but that it is important that the intensivist using POCUS knows his or her own limitations in ultrasound skills and asks for help if needed.3,6,20,25 POCUS and ‘normal’ ultrasound can therefore be seen as complementary; POCUS is not a replacement of a ‘normal’ ultrasound or other radiology modalities.
Weakness: On an individual level, there are still some colleagues in our hospital who are less enthusiastic about the intensive care department performing their own ultrasound exams; so far, this not resulted in serious conflicts. To date, no ultrasound-related incidents in direct patient care in our VIM database (hospital system for medical errors) have been registered.
2. TRAINING RESIDENTS
The Dutch Society for Internal Medicine has recently stated that POCUS is an obligatory element in the curriculum for internists (Landelijk opleidingsplan 2019). By designing a POCUS training program for intensive care residents, we combined both our own ambition to have staff and residents trained and the obligation to have Dutch residents in internal medicine trained in POCUS. Our aim is to have residents trained in POCUS before they start their intensive care rotation. Residents in internal medicine or its subspecialties in Rijnstate rotate through intensive care in their second year of residency and this rotation lasts 4-6 months. There are also residents in the Rijnstate Intensive Care Department who are not in training but do the same work as residents in training; on average, residents not in training stay in the department for one year. Residents not in training also participate in the POCUS course and are encouraged to use POCUS regularly. In the Rijnstate Hospital, the POCUS course is scheduled three times per year with the possibility to train 10 candidates each time. We started our course in 2017 and until now, have trained 64 residents, all courses are fully booked.
We decided that not only internists in training can be candidates for the course, and also ask residents who have an obligatory intensive care rotation (such as cardiology and pulmonology residents) to participate. This means that a far larger number of residents need to be trained. In Rijnstate, each year, five physicians start their internal medicine training program but the number of residents from other specialties is about five times higher. Key issues of POCUS curricula are becoming more clear but evidence about the precise content and duration of a training program is limited.26,27 In our view, only POCUS of the heart and lungs is insufficient as intensivists and internists are also confronted with acute abdominal pathology.28,29 We decided to combine basic thoracic and abdominal POCUS, and our view on the components of basic POCUS was recently published.13
3. TRAINING PROGRAM
The Rijnstate POCUS course for residents consists of three key areas,8 which will be described hereafter: a. image generation, b. image interpretation, and c. clinical integration.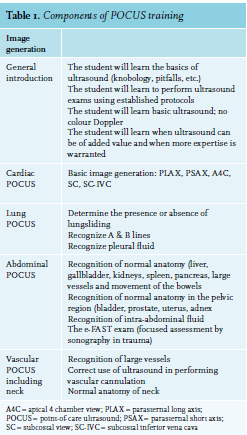
3.a. Image generation
After a general lecture on the theoretical background of ultrasound and possible pitfalls, the course participant is trained in acquiring the pre-defined appropriate images (table 1).
Short tutorials on every component of POCUS are followed by hands-on sessions under supervision in which the candidates use each other as mannequins. The morning sessions are under supervision of the radiology department and during morning hours, abdominal ultrasound is the main topic. The afternoon sessions are under responsibility of the intensive care and cardiology departments and during afternoon hours, the focus is thoracic ultrasound (heart and lungs). During the hands-on sessions, the number of candidates per ultrasound machine should be limited. In our experience, the optimal number of candidates per ultrasound machine and tutor is 3:1. The tutors should be experienced and qualified ultrasound experts.
The Rijnstate basic POCUS course consists of four days (Monday, Tuesday, Thursday, and Friday). Residents often have other educational obligations on Wednesdays so we have no fixed program on that day. We divided the several POCUS items over four days in a way we found appropriate for every POCUS item in terms of importance and or learning difficulty on the basis of available literature. Learning basic lung ultrasound is the quickest;30 learning cardiac and abdominal POCUS requires more time, but all elements of basic POCUS can be trained in a limited period of time.27,31,32 In table 2,.PNG) the time and number of test questions per POCUS item is shown. A two-day multi-organ POCUS training was efficient for intensive care fellows;33 others advise one day per application,34 but one-day courses are also described.35 Our four-day course gives ample time to soundly train POCUS and from a practical point, it means that residents have to be taken off rotation for one week.
the time and number of test questions per POCUS item is shown. A two-day multi-organ POCUS training was efficient for intensive care fellows;33 others advise one day per application,34 but one-day courses are also described.35 Our four-day course gives ample time to soundly train POCUS and from a practical point, it means that residents have to be taken off rotation for one week.
3.b. Image interpretation
During the course, the use of young healthy mannequins attributes to the element of image generation but the changes of finding pathology (image interpretation) are very low. Therefore, course participants learn to recognise normal ultrasound images and are instructed to be alert when images in patients are different from the normal images. During the introduction talks for each component, examples of ultrasound abnormalities are shown and the characteristics of ultrasound pathology discussed (table 3).
In the coming years, we foresee a bigger role for simulation education for ultrasound training as already has been described in literature,36 although simulation-only education is probably insufficient and hands-on training remains important.37 In the Rijnstate course, we use the Sonosim which is a computer-based platform in which ultrasound studies with real pathological situations are installed. Attached to the computer is an ultrasound probe with movement detection. By moving the ultrasound probe, different views are simulated. Candidates are therefore confronted with real ultrasound pathology. The candidates are stimulated to use the Sononsim during quiet hours. On the last day of the course, the candidates (in pairs) have to assess five Sonosim scenarios: cholethiasis, severe right and left ventricle dysfunction, E-fast protocol showing a pneumothorax on the right side, massive pulmonary embolism, and right kidney hydronephrosis. In the near future, we will explore whether we can optimise the use of ultrasound simulation. For the insertion of central lines, we use a vascular mannequin (Blue Phantom) on which the technique of ultrasound-guided catheterisation of the internal jugular vein can be practiced. In our department, residents are trained to insert central venous catheters into the internal jugular vein with ultrasound guidance, as endorsed in literature.38 This technique is part of the Rijnstate course but is rehearsed at the beginning of the intensive care rotation.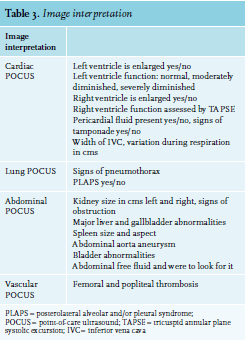
3.c. Clinical integration
Clinical integration of ultrasound findings is, in our view, the most difficult part. There are reports that physicians do not adequately maintain ultrasound competency after a basic course,39 and it is challenging to obtain specific recommendations from literature on maintenance of competency.19 The NVIC has designed a ‘consolidation course’, which includes, in addition to a two-day refresher of basic skills, the evaluation of 40 ultrasound examinations performed by the candidates within a period of nine months. These 40 thoracic ultrasound examinations are to be described according to the intracavitary ultrasound protocol (www.nvic.nl/ consolidatiecursus). In the near future, ultrasound portfolios for residents will be in place in our hospital, in which 40 ultrasound examinations (thoracic and abdominal) will be reviewed during a one-year period after the course. There is discussion on the exact number of ultrasound exams needed to reach acceptable competency,31 and for residents in internal medicine, an exact number will be replaced soon by the concept of entrustable professional activities (EPAs).11
Every Thursday afternoon at 3:00 p.m., there is an ultrasound round on the intensive care and general wards. Patients with interesting ultrasound findings are asked to participate and are examined by ultrasound by attending residents and one ultrasound supervisor.
By designing a basic POCUS course in combination with a one-year portfolio, the possibility to store exams digitally, weekly ultrasound rounds, and easy access to ultrasound supervision, we try to optimise the acquisition and retention of ultrasound skills. We fully endorse and emphasise the need to warn our residents that in the wrong hands, POCUS can be dangerous, and that it is essential to know one’s limits and to call for expert help if needed.3,4,24
Residents stay in Rijnstate for a maximum of one to three years, and after this period, they continue their training elsewhere. It will be up to them to maintain their POCUS skills and hopefully they will join a department with a positive POCUS attitude and program. The NVIC notices that just a small percentage of candidates from the basic course joins the consolidation course (data from NVIC, personal correspondence), meaning that most colleagues either stop performing POCUS after the basic course or continue with a personalised form of POCUS education (possibly ‘learning on the job’ without formal training).
3.d. Testing
The candidates are tested in theoretical and practical knowledge. An online theoretical multiple-choice test consisting of easy and more difficult questions with proportional percentage of questions for each component of POCUS (table 1) was developed. This test is taken shortly before the course to assess basic knowledge and candidate preparation, on the last day of the course to assess possible acquisition of knowledge, and after three months to assess whether the trained skills are retained by the candidates (learning retention). The questions and order of answers are changed digitally to prevent possible foreknowledge A practical exam is taken on the last afternoon of the course. The candidates are asked to show appropriate images of two lung, four heart, and four abdominal views in 10 minutes. They are evaluated in terms of speed, imaging quality, and ergonomics (table 4). This practical test is also rehearsed after three months to assess whether practical skills are retained. For intensive care fellows, a two-day multi-organ ultrasound course was found to improve ultrasound proficiency after three months.33 In a recent study on medical students, there was a difference in decay of motor and cognitive skills for pleural and cardiac images,40 meaning that we have to be aware that learning and retaining POCUS skills might be different for each component. We are planning to evaluate the results for our resident training program in 2020: Does our course improve ultrasound knowledge and skills, are knowledge and skills retained after three months, and is there a difference between retention of motor and cognitive skills? 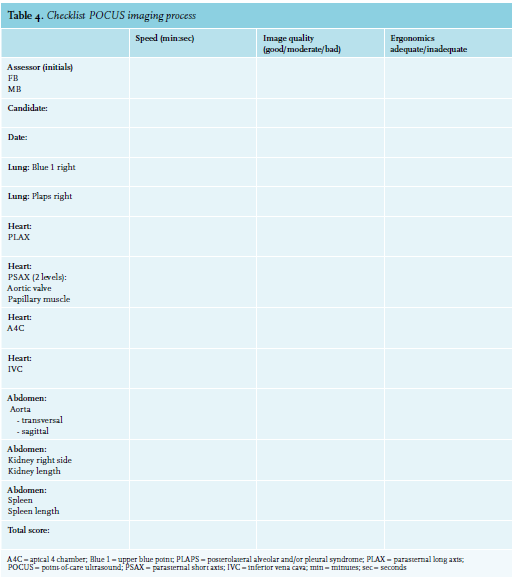
FINAL REMARKS
Although there is lack of hard evidence that ultrasound saves lives,41 we do strongly believe that POCUS is a very important new development in intensive care and emergency medicine. We are convinced that using it ‘as the new stethoscope’ leads to safer, better, and cheaper patient care. There is ample circumstantial evidence indicating that the use of POCUS leads to more accurate diagnosis, 42-52 has therapeutic implications,42,46,48,49,51-53 leads to lesser use of other medical resources,48,49,51,54,55 and probably leads to lower mortality.53,56
Furthermore, the use of POCUS may reduce uncertainty in the diagnostic process.49 From our experiences in our own clinical day-to-day work, we have encountered many situations in which the use of POCUS resulted in significant diagnostic and therapeutic alterations. Recently, we admitted a 45-year-old woman who suffered from a severe carbon monoxide (CO) intoxication. After several hours, her haemodynamic status deteriorated. POCUS not only showed a severe CO-related cardiomyopathy, but also showed a 20- week-old pregnancy, sadly without heart activity. We are sure that like us, colleagues who embrace POCUS will pass or have passed that point of no return when not using POCUS is just unimaginable.
In this paper, we describe our stepwise approach to implementing the integral use of POCUS and we also describe how a POCUS training program for residents could be designed. Of course, these topics are dynamic and require regular evaluation, improvements, and adjustments. By sharing our implementation and training experiences, we want to contribute to the spread of POCUS and be of help to colleagues who wish to implement POCUS into their intensive care departments.
REFERENCES