ABSTRACT
An 83-year-old man developed acute kidney failure after intra-articular use of gentamicin sponges for a periprosthetic hip infection. Haemodialysis was necessary for clearance of gentamicin, and for kidney function replacement. It is important to be aware that there is a risk of renal toxicity due to gentamicin when using a locally applied sponge.
KEY WORDS
Aminoglycoside, gentamicin, nephrotoxicity
INTRODUCTION
In systemic application of aminoglycosides, therapeutic drug monitoring (TDM) is necessary and considered usual care. This helps to achieve optimal dosage and intervals in order to achieve maximum efficacy and safety. High trough levels increase the risk of nephrotoxicity.2 TDM after the implantation of local gentamicin devices, such as beads and sponges, is not part of usual care. We describe an 83-year-old patient with toxic gentamicin concentrations, complicated by severe renal insufficiency. We also formulate an advice on how to prevent this in other patients.
CASE REPORT
An 83-year-old man was admitted with signs of acute periprosthetic joint infection. His medical history included hypertension and atrial fibrillation, and he used metoprolol 100 mg, chlortalidone 25 mg, quinapril 10 mg, and acenocoumarol. Symptoms were wound leakage and malaise. Leucocyte count was 11*10^9/l and C-reactive protein (CRP) was 57 mg/l. Treatment with flucloxacillin was started intravenously, and debridement of the hip with intra-articular placement of two 130 mg gentamicin sponges. In the four days following, the patient suffered from persistent malaise, vomiting, and mild hypotension (RR 100/50 mmHg). Antihypertensive medication was interrupted and intravenous fluid therapy was started. Despite this, the patient was progressively oliguric. Four days after the operation, laboratory tests revealed a gentamicin level of 2.6 mg/l, creatinine of 542 µmol/l, and estimated glomerular filtration rate (eGFR) of 8 ml/min. A previous creatinine value of 84 µmol/l was measured three months earlier. The patient had normal sodium and potassium values, calcium 1.91 mmol/l, and phosphate 2.28 mmol/l. No eosinophilia was found. Urinary analysis showed no proteinuria, only low leucocyte and erythrocyte counts, and no casts. Target value for gentamicin trough levels in our hospital is < 0.5 mg/l; in literature, a target value < 1.0 mg/l is also mentioned.2 We suspected acute tubular necrosis, on the one hand caused by gentamicin toxicity, and on the other hand by the moderately low blood pressure, which was related to infection and dehydration, and use of a thiazide and angiotensin converting enzyme (ACE)-inhibitor. Tubulo-interstitial nephritis caused by flucloxacillin was considered less likely, because of the very recent start of flucloxacillin and absence of typical abnormalities in urinary analysis. Post-renal obstruction was ruled out by ultrasound. Haemodialysis was started as renal function replacement therapy and to lower the gentamicin concentration in order to reduce further toxicity. Removal of the sponge was not possible due to degradation of these sponges within a few days. Gentamicin level decreased to 1.8 mg/l after starting intravenous fluid therapy and to 1.3 mg/l after the first dialysis session. Two days afterwards, plasma level had increased to 2.0 mg/l again while the fluid status of the patient had not changed. Dialysis was necessary on three consecutive days before gentamicin levels had decreased to a level of 0.7 mg/l. Sixteen days and six dialysis sessions after implantation of the sponge, the plasma concentration was still 0.6 mg/l. After five weeks, eGFR had recovered to 18 ml/min and dialysis was ended. After that, eGFR further recovered up to 50 ml/min.
DISCUSSION
With gentamicin sponges, high concentrations of gentamicin are achieved locally during approximately three days.3 The absorption of gentamicin in systemic circulation varies, but a study by Swieringa et al. demonstrates that concentrations in plasma generally drop below 2.0 mg/l within 24 hours and decrease after that.4 In the case we describe, the release profile of the sponge seems to deviate from the aforementioned profile. Extended release is suspected, based on the course of plasma concentrations, which were repeatedly increasing or at the same level as before the previous dialysis session (figure 1). Redistribution after dialysis must be considered, since Sowinski et al. shows a median gentamicin redistribution percentage of 38.7% after dialysis.5 Redistribution however, does not sufficiently explain the course of plasma levels in this patient, who exhibited levels still above 0.5 mg/l up to day 16.
The incidence of nephrotoxicity due to intravenously administered gentamicin is 10% to 25%.1 Accumulation of gentamicin in the tubulus cells leading to acute tubular necrosis is the most important mechanism of toxicity. This risk is increased in patients with nephrotoxic co-medication and hypotension. This case report demonstrates that locally applied gentamicin sponges may also cause toxic plasma levels and renal failure. The Netherlands Pharmacovigilance Centre Lareb reported one other case concerning toxic gentamicin levels and new renal insufficiency after the insertion of gentamicin sponges in a 73-year-old woman with an infected hip prosthesis. That patient needed to be treated with continuous veno-venous haemofiltration to limit loss of kidney function.6,7 Lareb also received four more notifications about patients with an increased creatinine blood level after insertion of gentamicin sponges to treat an infected hip replacement. Swieringa et al. describe a rise in serum creatinine in 10 out of 12 patients treated with gentamicin sponges, when using 4 to 6 sponges per patient.8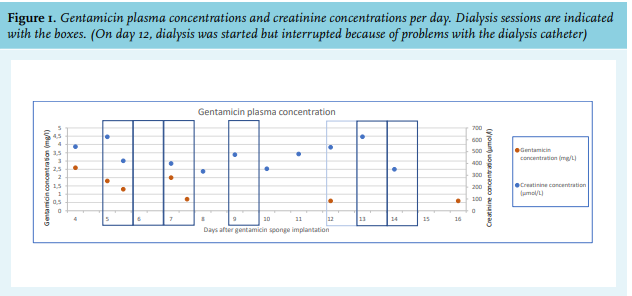
In order to treat gentamicin toxicity, it is important to discontinue gentamicin treatment, start supportive care by fluid administration, and to discontinue other nephrotoxic agents. Dialysis can be indicated for clearance of the causative agent, especially when using gentamicin sponges, since removal of the sponge is not possible. Acute tubular necrosis caused by gentamicin is often reversible, as was the case in our patient. Ototoxicity caused by gentamicin is often not reversible. In our patient, no objective tests of hearing and vestibular function were done since there were no subjective symptoms of ototoxicity.
After this case of intoxication, the monitoring of patients receiving gentamicin sponges and beads improved in our hospital: physicians must prescribe these materials via the electronic medication prescribing system. This enables extra monitoring by the pharmacist, who may suggest follow-up of creatinine and gentamicin levels, and in certain cases, may advise consultation by a nephrologist. Furthermore, this case led to increased awareness amongst physicians that measurement of eGFR is necessary before using local gentamicin sponges.
CONCLUSION
The use of gentamicin sponges may cause systemic toxicity. The release profile to the bloodstream of a gentamicin sponge is variable. Extended release of the sponge increases the risk of nephrotoxicity. Determination of eGFR is essential before deciding to apply a gentamicin sponge. If a sponge is implanted despite impaired renal function, extra attention to optimal fluid status and other nephrotoxic agents is necessary, as well as follow-up of eGFR and gentamicin levels after the procedure. Gentamicin sponges should be registered in the electronic prescribing system in order to facilitate extra monitoring.
REFERENCES