KEYWORDS
Evaluation, patient satisfaction, quality assessment, quality improvement.
INTRODUCTION
The Press Ganey survey is widely used in the United States to evaluate quality and performance of institutions and physicians. Some hospitals post the results of the survey online to allow patients to explore and select their potential providers. However, the Press Ganey survey is based on the subjective experiences of patients who may be prompted to respond based on a particularly positive or negative experience, and may have their responses modulated by unconscious biases. While data is unclear regarding the influence of physician sex on Press Ganey results, physician specialty choice and race do seem to impact the results, with non-white physicians tending to be rated lower than white physicians.1-4 If bias based on physician characteristics unrelated to medical competence – including sex, race, and specialty – influences Press Ganey results, then the survey results should either be corrected to account for bias, or use of the survey and wide dissemination of the results should be reassessed. The goal of this study was to compare results of the Press Ganey survey for physicians at two institutions and identify any physician factors, if present, that correlated with survey results.
METHODS
The compiled results of Press Ganey surveys posted online were collected for physicians at two hospitals: Wake Forest Baptist Health and Oregon Health & Science University. All physicians with a Press Ganey rating and a photograph were included in the study. Data was collected on physician sex, race, specialty, overall Press Ganey rating, and number and type of comments. Physician sex and race were determined by the author based on name, photograph, and country of origin if listed. Comment type was determined by the author and judged to be positive if the comment complimented the physician in any way or simply listed a positive word such as ‘good’ or ‘great’. Comments were judged to be negative if they criticised any aspect of the patient’s time with the physician. Comments that did not relate to the physician or complimented or criticised office workflow, staff, or wait times were not counted as positive or negative. Physicians were compared based on sex, race, and specialty on the basis of overall Press Ganey rating and comment type using Welch’s t-test with a significance level of 0.05. 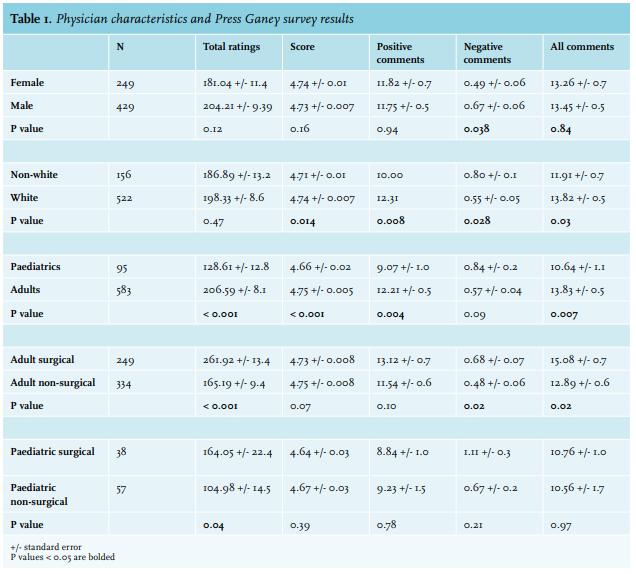
RESULTS
Included in the study were 678 physicians across two institutions. The majority were male (63.3%), white (77.0%), primarily treated adult patients (86.0%), and were in a non-surgical specialty (57.7%). The average Press Ganey rating was 4.73 out of 5; the average number of positive comments was 11.77; and the average number of negative comments was 0.60. As shown in table 1, when compared on the basis of sex, female physicians had a lower average number of negative comments (0.49 female vs. 0.67 male, p = 0.04). No difference was found in average number of ratings (181.0 female vs. 204.2 male, p = 0.12), average rating (4.74 female vs. 4.73 male, p = 0.16), average positive comments (11.8 female vs. 11.8 male, p = 0.94), and average total comments (13.3 female vs. 13.5 male, p = 0.84).
When compared by race, white physicians had higher average ratings than non-white physicians (4.74 white vs. 4.71 non-white, p = 0.01), greater number of positive comments (12.3 white vs. 10.0 non-white, p = 0.008), fewer negative comments (0.55 white vs. 0.80 non-white, p = 0.03), and more comments overall (13.8 white vs. 11.9 non-white, p = 0.03).
When broken down by specialty, physicians in any paediatric specialty had on average, fewer ratings (128.6 paediatrics vs. 206.6 adults, p < 0.001), lower ratings (4.66 paediatrics vs. 4.75 adults, p < 0.001), fewer positive comments (9.07 paediatrics vs. 12.21 adults, p = 0.004), and fewer total comments (10.6 paediatrics vs. 13.8 adults, p = 0.007).
Physicians in adult surgical specialties tended to have more ratings (261.9 surgical vs. 165.2 non-surgical, p < 0.001), more total comments (15.1 surgical vs. 12.9 non-surgical, p = 0.02), and more negative comments (0.68 surgical vs. 0.48 non-surgical, p = 0.02). Physicians in paediatric surgical specialties also had more comments on average (164.1 paediatric surgical vs. 105.0 paediatric non-surgical, p = 0.04). There was no significant difference in average rating for surgical or non-surgical specialties, though non-surgical specialties in both adult (4.73 surgical vs. 4.75 non-surgical, p = 0.07), and paediatric (4.64 surgical vs. 4.67 non-surgical, p = 0.39) practices tended to have slightly higher ratings.
DISCUSSION
The findings of this study suggest that physician characteristics influence Press Ganey survey results. In particular, physician race (white vs. non-white) and specialty choice may have a positive or negative effect on the survey. Physician sex did not appear to affect survey results in this study.
Although there is limited data on the influence of physician characteristics on the Press Ganey survey, this study supports others that have found a bias favouring white physicians and no effect of physician sex, though the latter remains controversial.1,3,4 A 2018 cross-sectional study of outpatient gynaecology visits found that female gynaecologists were rated significantly lower than their male counterparts due to their sex alone.2 However, a 2017 retrospective observational study found no association between physician race and sex and Press Ganey rating, although white physicians were consistently rated higher and male physicians scored higher than females in certain categories.1 This 2017 study also found that physician specialty influences Press Ganey ratings, with obstetricians scoring highest followed by surgeons.
To the author’s knowledge, the current study is the first that examines the differences in Press Ganey ratings between physicians in adult and paediatric specialties. The lower average ratings for paediatric specialties may occur because the parent is often completing the survey rather than the patient, and the parent may be more likely to take offense on behalf of their child if a perceived slight occurred. Physicians and parents also often have differing interpretations of what a child’s medical needs are, and misunderstandings could lead to lower ratings.5 For example, a parent observing a physician examining their sick child may be concerned that the physician is upsetting the child or being too aggressive, which could translate into parental dissatisfaction with the physician and subsequent low Press Ganey ratings.
While physician race seems to consistently influence Press Ganey ratings across specialties, sex may have an effect on some specialties more than others, and its effects may need to be analysed on a specialty-byspecialty basis. Regrettably, the race bias that appears to exist across specialties, and the sex biases that may or may not be present, likely represent symptoms of biases and stereotypes present in society as a whole, and thus medicine is unlikely to single-handedly eliminate patient bias towards physicians of particular characteristics. Medicine may be more successful at combatting specialtyspecific bias, as there are no competency reasons for why obstetricians or adult specialists should be rated higher than any other type of physician. The origin of these apparent biases may be due to the types of environments in which physicians work and the patient emotions often present there. Obstetricians are part of an often-joyous occasion, and patients’ positive feelings towards the event may translate into positive feelings towards their physician. Likewise, patients may have high regard for surgeons, who are often able to affect dramatic cures or immediate improvements in quality of life. Visits with the internal medicine physician whose treatments take time with often gradual effects, as well as the paediatrician, with whom visits may seem a formality for a healthy child, likely evoke fewer strong positive emotions and thus perhaps a lower rating. Separating patient satisfaction with the physician from patient feelings towards the visit or their condition may be difficult to impossible, but possible measures could include distributing surveys several weeks or even months after the visit so that any strong emotions surrounding the visit have cooled; or conversely distributing the survey immediately after the visit so that a patient does not forget about an ordinary but satisfactory visit.
That physician specialty and race appear to influence Press Ganey survey results suggests that the survey may not be as unbiased as it was intended to be, and that its results should not be used as a marker of a physician’s skill at his or her job. Given that the average patient is unlikely to select a physician by comparing ratings within a physician’s particular demographic group (e.g., white female paediatric neurologists), it would seem best to remove Press Ganey ratings from public view to avoid selection of a physician based on potentially biased results. These study results also call into question the utility of the Press Ganey survey to institutions as well. While portions of the survey may be useful in identifying system-wide problems, such as long wait times or poor coordination or communication between services, given the apparent bias in the survey results, institutions should rethink forming judgments on an individual physician’s competence using Press Ganey results, and that perhaps the survey should remove such questions altogether. Other options to evaluate physician skill could include objective measures, such as incidence of post-operative complications for surgeons, or percentage of patients who have achieved blood pressure or haemoglobin A1c level goals. An example of this is the Medicare Access and Children’s Health Insurance Program (CHIP) Reauthorization Act Merit-based Incentive Payment System, which provides financial incentives and penalties for various measures of healthcare quality.6 Subjective measures of evaluation could include distributing surveys to not only patients but also support staff and other physicians to gain a better understanding of how a particular physician works with his or her colleagues.
Limitations of this study include inclusion of only two institutions and the subjective judgement by the author of comments as positive or negative. There was also minimal to no representation of certain specialties, such s pathology, radiology, hospital medicine, and emergency medicine, due perhaps to lack of distribution of surveys to hospitalised patients, low response rates, or minimal direct patient contact. Future directions include inclusion of more institutions and inclusion of more specialties.
The widely used Press Ganey survey may not be free from bias, as demonstrated by non-white physicians and physicians in paediatric specialties scoring lower than their white and adult specialty counterparts. These findings suggest that evaluation of a physician’s competence based on the Press Ganey survey is not valid and that the survey should be redesigned, or perhaps that questions relating to the physician should be removed from the survey entirely to better facilitate improvement of an institution as a whole.
DISCLOSURES
The author declares no conflicts of interest. No funding or financial support was received.
REFERENCES