KEYWORDS
Chloroquine, poisoning, intravenous lipid emulsion, intraosseous, alkalinisation, sodium bicarbonate, diazepam
INTRODUCTION
In Western countries, prescription drugs are used in about 90% of suicide attempts with drugs.1 In some countries, chloroquine is used in suicide attempts.2 Chloroquine has a strong membrane-stabilising effect and intoxication may present with neurological, cardiovascular, respiratory, and digestive symptoms. We describe a patient with haemodynamic stabilisation after empiric treatment for intoxication with QRS widening, which turned out to be due to chloroquine. Intraosseous administration of lipid emulsion failed to improve haemodynamic parameters in this case.
CASE REPORT
At home, a 27-year-old female called the emergency number and reported a suicide attempt with medication. Prescribed medicines were clonidin, dextroamphetamine, flurazepam, and promethazine. A few hours after admission, her family reported that she frequently bought medicines online. Upon arrival of the paramedics, she was fully conscious with normal vital signs. While entering the ambulance she became asystolic and cardiopulmonary resuscitation (CPR) was performed for 19 minutes. She was intubated on the scene.
Upon arrival in the emergency department, very broad QRS complexes (326 ms) were observed. An overdose with her prescribed medicines would not cause QRS widening and aside from flumazenil for flurazepam, no specific antidotes are available. Because of the combination of an unknown intoxication and widened QRS complexes, sodium bicarbonate 100 ml 8.4% and intravenous lipid emulsion (ILE) 20% (100 ml bolus followed by 400 ml infusion) were given via intraosseous infusion. Shortly after arrival, she lost circulation and CPR was restarted according to protocol with addition of intraosseous 950 mg calciumgluconate. The possibility of extracorporal life support was considered, but due to distance and time to start of perfusion, this seemed impossible.
Despite the therapy mentioned above and the start of vasopressors, circulation remained unstable and the patient experienced a total of three cardiac arrest episodes in the hospital due to pulseless electrical activity. As further alkalinisation would aggravate an already very severe hypokalaemia (1.5 mmol/l; reference: 3.5-5 mmol/l), we decided to repeat the full dose of lipid emulsion intravenously as a last possible resort (cumulative dose of 15 ml/kg). Shortly thereafter, haemodynamic parameters and cardiac contractility improved. Toxicological analysis showed a high level of chloroquine (16.1 mg/l three hours after ingestion; reference for toxic level: > 0.5 mg/l) and a positive blood test for benzodiazepines. High-dose diazepam was added, resulting in further improvement of cardiac contractility and the possibility to cease vasopressor agents. Alkalinisation was restarted as soon as potassium stabilised with supplementation; active charcoal was administered repeatedly (total dose of 150 g). After 60 hours, cardiac conduction normalised and therapy with sodium bicarbonate and diazepam was discontinued. Figure 1 shows the timeline of events after ingestion of the overdose of chloroquine. On day seven, the patient was extubated. She made a full recovery from the post-anoxic and toxic encephalopathy. 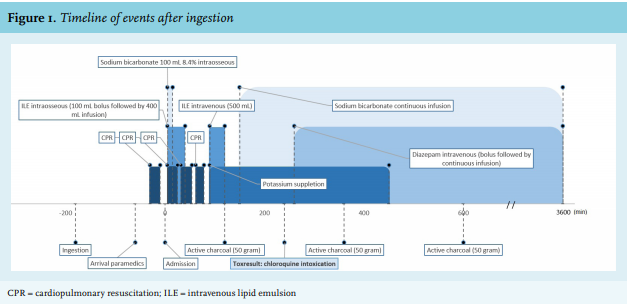
DISCUSSION
In the Netherlands, chloroquine is rarely prescribed and is unavailable over the counter. In this case, chloroquine was ordered via an internet pharmacy with the intention to commit suicide.
Since the study of Riou et al,3 patients with chloroquine intoxication are almost always treated with early mechanical ventilation, and a high dose of diazepam and (nor)epinephrine.2 Although definitive evidence for effectiveness of this approach is lacking, we followed this regimen in our patient. Furthermore, we administered active charcoal since chloroquine is a carbon-absorbable molecule.4
Because the ingested substance was initially unknown, we started treatment with sodium bicarbonate because of a widened QRS complex. Sodium bicarbonate is widely used to treat toxin-induced sodium channel blockade, as alkalinisation leads to increased protein binding of the sodium channel-blocking drug. Data of its use in chloroquine poisoning are limited. Since the focus has been on the therapy described above, sodium bicarbonate administration alone is never tested for its efficacy. The most important complication of sodium bicarbonate is hypokalaemia due to intracellular shifting. This is of utmost importance in chloroquine overdose, since one of the features of severe chloroquine intoxication is hypokalaemia, as was the case in our patient.5,6
Chloroquine is a highly lipophilic substance; thus, administration of lipid emulsion in case of life-threatening symptoms seems rational. There is little evidence supporting the use of intravenous lipid emulsion (ILE) in (hydroxy)chloroquine intoxications. One report presents temporary return of spontaneous circulation in cardiac arrest due to chloroquine poisoning after administering ILE 20% (1.5 ml/kg bolus followed by 0.25 ml/kg/min infusion) in one patient.7 Two other patients were successfully treated with the same dosing regimen of ILE within two hours after suicide attempts with hydroxychloroquine. Both patients were concurrently treated with sodium bicarbonate and diazepam, and vasopressor agents were used in one of them.8 However, two cases without benefit of ILE were also reported in literature. In the first case, infusion of ILE was started 11 hours after ingestion, in the second case, the ingested dose of hydroxychloroquine was extremely high.9
Very few data about intraosseous administration of lipid emulsion exist. An animal study did not show any difference in time to recovery of haemodynamic variables after intravenous bupivacaine injection in rats treated with intraosseous lipid emulsion versus intravenous administration.10 Sampson and Bedy11 describe a patient with massive verapamil overdose who received part of the lipid emulsion through an intraosseous line. Administration was limited due to a flow alarm after 60 ml and by that time, intravenous access was established so therapy was moved to that site. The patient died two days after admission. There is one description of successful treatment of seizures after intraosseous injection of lidocaine with intraosseous lipid emulsion in an 11-month-old male.12
In the case, we describe that the first dose of ILE was given intraosseous infusion and did not achieve any haemodynamic improvement. Since haemodynamic parameters stabilised and cardiac contractility improved after a second, intravenous dose, we hypothesise that the first dose remained in the bone marrow compartment. There was no flow alarm during infusion of the intraosseous dose and, since we monitored pulsatile output on the catheter in the radial artery and a normal pulse oximetry plethysmographic waveform was seen during CPR, lack of efficiency due to low output does not seem to be the explanation either. Although we cannot exclude the possibility that the first intraosseous dose of lipid emulsion was too low to bind a substantial part of the chloroquine, we recommend that physicians be aware of the possibility that intraosseous lipid emulsion might be less effective and to avoid intraosseous administration of lipid emulsion. Further research on the pharmacokinetics of intraosseous administration of lipid emulsion is necessary.
CONCLUSION
We were challenged with a severe intoxication with chloroquine that was bought online. Successful treatment with sodium bicarbonate and ILE was started before the substance was identified. In our patient intraosseous administration of lipid emulsion was ineffective, compared to intravenous administration.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received. This case was previously presented as a poster presentation at the 38th congress of the European Association of Poisons Centres and Clinical Toxicologists (EAPCCT) held in Bucharest (May 22-25th, 2018).
REFERENCES