DIAGNOSIS
X-ray and CT scan of the chest showed extensive small-sized calcifications of the spleen (figure 1).
Various autoimmune disorders can cause splenic abnormalities, like splenomegaly and splenic infarction. SLE is a chronic multisystemic autoimmune disease, in which several organs and tissues are damaged by pathogenic autoantibodies and immune complexes. Abdominal involvement of SLE can occur in virtually any organ within the abdominal cavity, although only renal involvement integrates diagnostic criteria.1 Rupture, splenomegaly, infarction, infections, and atrophy of the spleen have been recognized in patients with SLE. Rapid enlargement of the spleen in a lupus patient should raise concern for the possibility of lymphoma.2
Splenic calcifications have been reported in SLE and in various other diseases such as rheumatoid arthritis, systemic sclerosis, amyloidosis, sickle cell anaemia, anthracosilicosis, lymphoma, infections (histoplasmosis, tuberculosis, brucellosis, candidiasis, Pneumocystis jirovecii), trauma and coeliac disease.3-5 Despite this wide range of causes, splenic calcifications still remain rare and reports on prevalence are not available. In our case, these other causes of splenic calcifications like infections (negative HIV testing, interferon gamma-release assay – tuberculosis negative), sickle cell anaemia, lymphoma and environmental causes were ruled out from the history, clinical examination and laboratory findings. Segmental splenic infarction associated with lupus anticoagulants and anti-cardiolipin antibodies can also result in splenic calcification, however were negative in our patient. Whether splenic calcification can predispose to hyposplenism remains unclear.3 It may precede autosplenectomy and hyposplenism, possibly emphasizing the importance of pneumococcal vaccination.6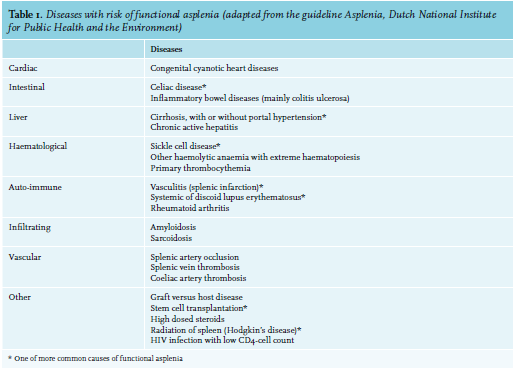
The guideline on hyposplenism from the ‘Dutch National Institute for Public Health and the Environment’ recommends vaccination and antibiotics for patients with sickle cell disease, splenic infarction and radiation of the spleen. In other diseases able to cause functional hyposplenism (table 1) like SLE, this is less clear. Peripheral blood smear without Howell-Jolly bodies does not exclude functional hyposplenism, and ultrasound and CT imaging is inefficient to judge splenic function. Spleen scintigraphy could be conclusive, but is invasive. So, in these cases, the advice to treating medical specialists is to not routinely provide vaccination and antibiotics to all patients with potential hyposplenism, but to individually assess each case in consultation with an infectious diseases consulant.7
DISCLOSURES
The authors have no conflicts of interest to declare.
REFERENCES