DIAGNOSIS
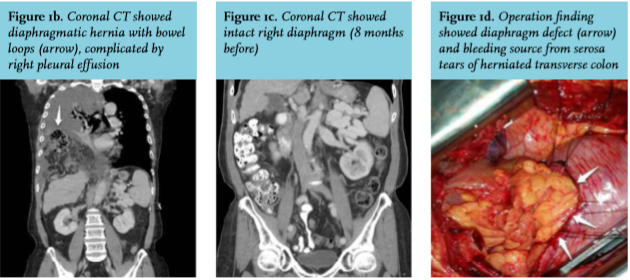
Computed tomography showed massive right pleural effusion and right diaphragmatic hernia (DH) (figure 1b). The computed tomography done eight months ago showed an intact diaphragm (figure 1c). The thoracic surgeon was consulted because of suspected strangulation of the colon with septic shock. Emergency thoracotomy was performed, which disclosed a massive hemothorax caused by a serosa tear of herniated transverse colon (figure 1d). No ischemic change of the colon was noted. Both the colonic and diaphragmatic defects were repaired. The postoperative course was uneventful.
Late DH secondary to radiofrequency ablation (RFA) is an uncommon phenomenon. RFA complications are subdivided into four categories: thermal damage from heating and mechanical, septic, and other unexplained causes.1 The main reason for DH after RFA is diaphragmatic injury secondary to thermal damage. There are several precipitating factors, including tumor adjacent to the diaphragm, poor liver function and cirrhosis, all of which weaken the diaphragm.2 Early symptoms such as nausea, vomiting, and post-prandial abdominal pain are nonspecific, which makes early diagnosis difficult. When abdominal organs herniate into the pleural cavity, this may cause right upper quadrant pain, dyspnea, pleural effusion or strangulation of the bowel which in turn can result in septic shock.2 Diagnosis using plain radiographic examination includes visualization of abdominal organs in the chest, lack of clarity of the hemidiaphragm, or abnormal nasogastric tube positioning. Contrast-enhanced computed tomography plays an important role in the diagnosis and in determining whether the intruding abdominal organs are necrotic. Conservative treatment may be chosen in selected stable patients. Definite treatment is surgical repair, either open or laparoscopic.3 To prevent thermal injury induced by RFA, artificial ascites or intraabdominal carbon dioxide, insufflation before RFA to separate the hepatic tumor and diaphragm is warranted as an effective method.4
In addition, hemothorax related to DH often occurs in traumatic patients. In this case, the cause of hemothorax may be related to mechanical injury from friction between the defect of the diaphragm and the herniated colon. However, most patients presenting with shock are in shock because of sepsis originating from strangulation of the bowel and not because of haemorrhage. In conclusion, DH is a rare late complication of RFA and herniation of the colon can lead to hemothorax. Hemothorax is most often of traumatic origin. When a patient presents with shock and herniated diaphragm, the first thing to check for is sepsis; nevertheless, hypovolemic shock from hemorrhage of herniated organ should still be in the differential diagnosis.
REFERENCES