KEYWORDS
Hypothyroidism, renal injury, iodine ablation therapy, thyroid hormone withdrawal
INTRODUCTION
Thyroid hormones have a direct effect on almost all body organs. The interplay between thyroid hormone and the kidney is complex. Thyroid hormone directly affects the normal growth and development of the kidney and the kidney in turn has effects on thyroid hormone metabolism and elimination.1,2
Thyroid hormone is also known to cause changes in hemodynamics, which in the kidney is mediated by changes in the renin-angiotensin-aldosterone system (RAAS) and alterations of the excretion of electrolytes and water.3 In overt hypothyroidism these effects, along with decreased cardiac output and increased vascular resistance, can cause decreased renal blood flow with a subsequent decrease in glomerular filtration rate (GFR).4,5 In some cases of severe hypothyroidism, reversible acute kidney injury is reported. However, the exact incidence of acute kidney injury in hypothyroidism remains unknown.
Although elevated creatinine due to hypothyroidism has been described in a number of observational studies and case reports, screening for hypothyroidism is not included in the routine workup of acute kidney injury and thus physicians are generally unfamiliar with this phenomenon. As a reminder for clinicians to consider hypothyroidism in the differential diagnosis of acute kidney injury, we offer a case of subacute kidney injury due to hypothyroidism which led to unnecessary hospital admission and diagnostics.
CASE REPORT
A 59-year-old man was referred to our clinic with a nodular mass of the thyroid. His medical history consisted of depression and gastroesophageal reflux disease for which duloxetine and omeprazole had been prescribed. Anamnesis yielded no relevant findings, besides hoarseness during the last two weeks. The nodular mass of the thyroid was classified as TIRADS-4a, corresponding to a 5-10% chance of malignancy. After biopsy and hemithyroidectomy, the patient was diagnosed with multifocal papillary thyroid carcinoma (TNM stage: T1bN0M0). Patient was scheduled for completion thyroidectomy and radioiodine-131 (I-131) ablation therapy eight weeks after surgery. In accordance to the Dutch guideline levothyroxin therapy was withheld prior to the ablation therapy, resulting in severe hypothyroidism with a thyrotropin above 50 mU/l (assay specific upper limit of detection: 50 mU/l, reference range: 0.3-5.6 mU/l) and an undetectable level of thyroxin. Due to logistic errors, the total time of thyroid hormone withdrawal was eight weeks, which is four weeks longer than recommended by the Dutch guideline.
During thyroid hormone withdrawal, the creatinine level rose to a maximum of 152 μmol/l (reference range: 60-110 μmol/l). Prior to completion thyroidectomy, the creatinine level had been stable at 78 μmol/l. The combination of increased serum creatinine and general discomfort with fatigue and muscle aches being the main complaints, the nephrologist was consulted, who decided to admit the patient to the hospital for further examination. At this time, the patient had been on thyroid hormone withdrawal for seven weeks. Upon admission, there were no signs of inadequate fluid intake or fluid loss. Physical examination showed no change in body weight nor peripheral oedema. At the time of admission there were no signs of hypotension (blood pressure on average 155/85 mmHg) or oliguria. Urine analysis revealed no erythrocyturia, leukocyturia or proteinuria. Post renal obstruction was ruled out by ultrasonography. Omeprazole was the only nephrotoxic medicine prescribed at the time. However, tubulointerstitial nephritis was deemed unlikely due to the chronic use of this drug and absence of other clinical signs such as eosinophilia, leukocyturia or proteinuria. Furthermore, after discontinuation of omeprazole, a further increase of creatinine was observed. The patient was discharged after two days without any changes in creatinine clearance, as at that point hypothyroidism induced kidney injury was suspected. One week later I-131 ablation was performed and hormone replacement therapy (HRT) with levothyroxine was initiated. Four days after HRT was initiated, his creatinine value had decreased to 102 μmol/l and eventually decreased further to preoperative values (figure 1).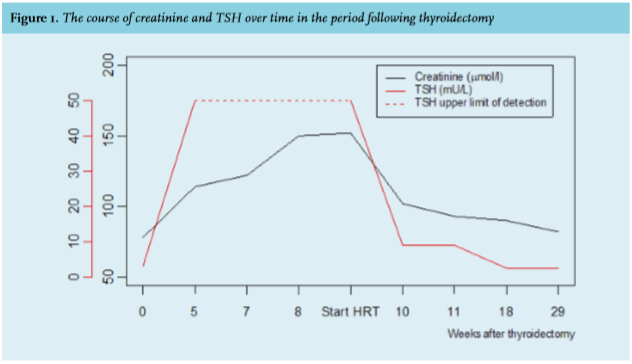
DISCUSSION
This case report describes a patient with subacute kidney injury due to hypothyroidism after thyroidectomy awaiting ablation therapy with radioactive iodide, which seemed fully reversible after initiation of thyroid hormone substitution. The relationship between hypothyroidism and elevated creatinine was first described in 1957.6 Since then, several observational studies and case series have summarized the biochemical abnormalities that occur with hypothyroidism, and their reversibility after initiation of hormone replacement therapy. Through PubMed, MEDLINE was searched for prospective studies evaluating the change in renal function in hypothyroidism before and after treatment with thyroid hormone. A summary of available literature is given in table 1 including articles in English published after 1990. 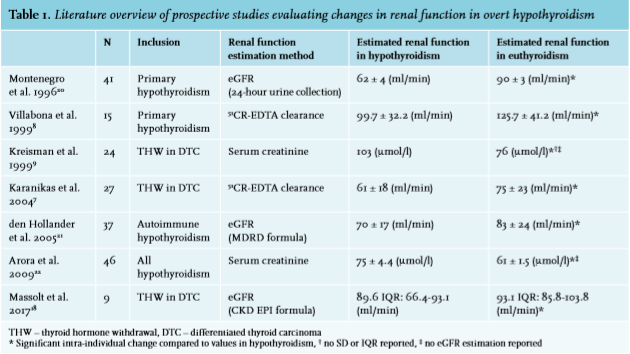
These prospective studies all measured significant deterioration in renal function in consecutive hypothyroid patients, independent of the method used to estimate renal function. It has been suggested that elevated creatinine in hypothyroidism is fully attributable to increased muscle breakdown. This hypothesis is contradicted by the studies evaluating renal function through non-creatinine dependent methods7,8 and studies showing elevated creatinine in the absence of substantial increase of creatine kinase.9
Nevertheless, there are multiple other mechanisms that explain the elevation of creatinine in hypothyroidism. First, hypothyroidism induces alterations in the transcription of gene products in the cardiomyocyte leading to diminished production of Ca2+-ATPase and changes in expression of phospholambam, which is a protein regulating Ca2+-ATPase activity in the sarcoplasmic reticulum of the cardiomyocyte. These alterations decrease myocyte contractility and have been shown to decrease systolic function as well as impair diastolic relaxation of the myocardium.4 Second, hypothyroidism causes an increase in vascular resistance due to impaired dilatation of the endothelium.10,11 The combination of these cardiovascular effects is thought to cause a decrease in renal blood flow and decrease glomerular filtration rate.
Also, renal auto regulation may be impaired by decreased sensitivity to beta adrenergic stimuli and decreased production of renin, therefore reducing the action of the renin-angiotensin system.3 Finally, thyroid hormones also affect the proximal tubule in the kidney. Hypothyroidism leads to impaired water and sodium reabsorption due to decreased expression of mRNA coding for alpha and beta subunits of Na+/K+-ATPase, decreasing blood volume.12 A subsequent decrease in GFR is reported, presumably caused by vasoconstriction of the afferent renal arteriole due to a tubule-glomerular feedback system response to filtrate overload.13
Although creatinine elevation is common in hypothyroidism, a near doubling of the serum creatinine as in this case was not reported in the prospective studies. However, more severe kidney injury is a rare consequence of hypothyroidism and is mostly caused by rhabdomyolysis, which has been reported as a cause in most but not all case reports.14-17 Creatine kinase levels were not measured in our patient. Therefore, rhabdomyolysis cannot be excluded as the cause of acute kidney injury, although the absence of urine abnormalities does not suggest rhabdomyolysis.
In this report, due to logistic errors the duration of hypothyroidism was eight weeks, whereas a period of four weeks is recommended by the Dutch guideline. It is likely that prolonged exposure to hypothyroidism was the cause of the marked increase of creatinine. Figure 1 shows that creatinine increased linearly over time. In contrast, Karanikas7 and Massolt18 did not show significant further increases in serum creatinine values after five and four weeks of thyroid hormone withdrawal, compared to the two weeks of withdrawal in the study by Kreisman.9 However, the relationship between renal function and time dependent exposure to hypothyroidism has not yet been systematically studied.
In future cases where a patient is expected to be exposed to a prolonged state of hypothyroidism (e.g. longer than the four weeks recommended by the Dutch guideline), a physician should consider expediting I-131 ablation therapy and initiation of thyroid hormone substitution or consider the use of recombinant TSH, especially in cases at risk, such as those with pre-existing chronic kidney disease. In addition, screening for hypothyroidism is recommended in cases of elevated creatinine of unknown aetiology.
As a final note, even though creatinine fell back to prior values, it is important to note that a temporary deterioration of renal function has been associated with an increased risk of chronic kidney disease and mortality.19 Therefore, it does not seem fit to interpret such events as harmless.
In conclusion, hypothyroidism is an easily overlooked cause of renal impairment. Awareness of this phenomenon can avoid unnecessary hospital admission and costly diagnostic procedures.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES