Full textPDF
Full text
CASE REPORT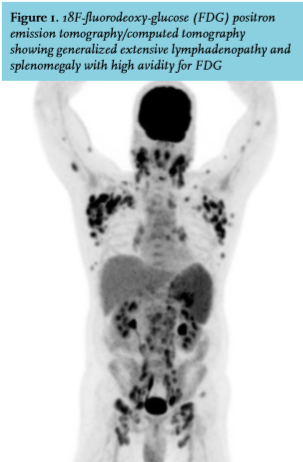
A 54-year-old man, originally from Sri Lanka, was admitted to our hospital with fever, night sweats and enlarged axillary lymph nodes. His medical history included human immunodeficiency virus (HIV) infection, diagnosed three years prior to presentation, with a CD4 count of 27/ul (CDC C3), primary syphilis, candida esophagitis, cytomegalovirus retinitis and psychosis. Medication consisted of emtricitabin, tenofovirdisoproxil, duranavir and ritonavir. Six months before presentation medication had been changed to emtricitabin, tenofovirdisoproxil, elvitegravir and cobicistat, after which CD4 count rose from below 100/μL to above 200/μL. For the past two months he had been complaining of tiredness, coughing and fever. Physical examination revealed no abnormalities other than enlarged axillary and cervical lymph nodes. Laboratory investigation showed a C-reactive protein level of 70 mg/l and a chest X-ray was unremarkable. His CD4 count and viral load were 220/μL and 20 copies/ml, respectively. A 18F-fluorodeoxy-glucose positron emission tomography (FDG PET) combined with a computed tomography (CT) scan was performed (figure 1).
WHAT IS YOUR DIAGNOSIS?
See page 307 for the answer to this photo quiz.