KEYWORDS
Glucarpidase, methotrexate, toxicity
INTRODUCTION
Methotrexate (MTX) is an important chemotherapeutic agent for many oncological indications. MTX disrupts cell repair and proliferation by inhibition of folate reduction through the dihydrofolate reductase enzyme in both malignant and healthy cells. Reduced folates are used as cofactors in DNA and RNA synthesis.1,2 High-dose MTX therapy, generally defined as > 500-1000 mg/m2 , is therefore followed by administration of leucovorin to counteract the effects of MTX on healthy cells. Leucovorin itself is a reduced folate, bypassing the inhibition of MTX and reducing its cytotoxic effects. High-dose MTX therapy carries the risk of acute kidney injury (AKI) by precipitation of MTX in the renal tubules.1 Volume depletion and acidic urine are major risk factors for MTX precipitation. Therefore, hyperhydration and urine alkalinisation are vital parts of MTX treatment protocols. MTX-induced AKI has the potential to induce a vicious circle in which delayed clearance maintains high systemic MTX levels, in turn causing further kidney injury. Sustained high systemic levels of MTX may lead to myelosuppression, hepatic and pulmonary toxicity, neurotoxicity and Stevens-Johnson syndrome. Toxicity plasma concentration thresholds vary based on the organ system, but it has been reported there is a greater risk for toxicity with plasma levels greater than 10 µM at 24 hours. Empirically developed nomograms are often used 24 to 36 hours post infusion to determine if patients are at high risk for MTX toxicity and to pharmacokinetically guide leucovorin rescue therapy based on the MTX serum concentrations and the time post MTX infusion.1
Here we describe a case of MTX intoxication in which standard supportive therapy was complemented by glucarpidase, a relatively novel treatment for MTX intoxication. We then review the available evidence to support this treatment.
CASE REPORT
A 39-year-old male with a history of Crohn’s disease was admitted to our ICU with increased serum creatinine (from 66 to 398 µmol/l) and MTX levels (23 µmol/l) 70 hours after high-dose (5 g/m2 ) MTX for acute lymphoblastic T-cell lymphoma, despite preventive measures including leucovorin, intravenous hydration and urine alkalisation. Leucovorin therapy was intensified based on treatment protocols as described in the HOVON 100 ALL trial,3 while vigorous hydration and urine alkalisation were continued.
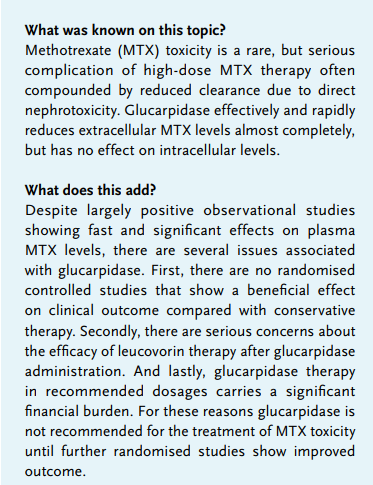
Because of progressive renal failure under maximum supportive therapy, addition of glucarpidase was considered at admission. Glucarpidase was ordered from Clinigen Healthcare Ltd. in the United Kingdom and was delivered to our hospital the next day. Eighty-five hours after initiation of MTX treatment, serum MTX levels had decreased to 12 µmol/l. Glucarpidase was administered in a single dose of 50 IU/kg and within one hour the serum MTX level had decreased to 0.10 µmol/l (figure 1).
In the days after glucarpidase treatment a small, but significant rise in serum MTX levels to a maximum of 0.63 µmol/l was noted. Creatinine levels remained elevated (figure 1). In the following days, the patient received two sessions of haemodialysis with a minimal effect on the serum MTX level at a sieving coefficient of 0.08.
The patient was discharged to the general ward. His renal function improved in the following weeks and after one month his estimated glomerular filtration rate (eGFR) had normalised to pre-toxicity levels. Four months later a PET-CT scan showed complete remission. 
DISCUSSION
MTX intoxication is a life-threatening complication of high-dose MTX. Its incidence has decreased after the introduction of MTX treatment protocols that include screening for third space fluid collections such as ascites and pleural fluid, intensive hydration and alkalinisation, and leucovorin therapy. Once this complication occurs, however, it still carries a high risk for severe morbidity and mortality. The goal is to treat the effects that have already occurred and to minimise further toxicity. Our patient received glucarpidase in addition to intensified leucovorin rescue treatment, hyperhydration and urine alkalisation, and recovered.
Extracorporeal techniques such as haemofiltration and haemodialysis have been used to enhance MTX clearance. Evidence for the efficacy of these techniques is mostly limited to case reports with varying efficacy.4-13 High-flux haemodialysis is thought to be most effective in removing MTX. With all extracorporeal techniques a significant rebound effect necessitating multiple treatments often occurs.14 The risks of these techniques are haemodynamic instability and introduction of invasive catheters in patients prone to infection and bleeding diathesis.
Recently, glucarpidase has come under attention as an alternative to extracorporeal techniques. Glucarpidase, or Voraxaze™, is a carboxypeptidase that can eliminate extracellular MTX by hydrolysing its terminal carboxylglutamate residue, producing inactive metabolites such as 4-deoxy-4-amino-N10-methylpteroic acid (DAMPA).15 Four case series reported an important reduction in extracellular MTX levels in adult patients after a single dose of glucarpidase.16-19 Widemann et al. performed a pooled analysis of efficacy data from these four multicentre, single arm, compassionate use clinical trials using protocols from 1993-2007.20 This analysis showed that glucarpidase can rapidly and safely reduce extracellular MTX levels by a median of 99% and a clinically important reduction in 59% of patients. Side effects of glucarpidase treatment, while difficult to distinguish in patients with symptoms of MTX toxicity, were rare and self-limiting in all of the case series. Paraesthesia and flushing were most often reported. The effects of glucarpidase on intracellular concentrations of MTX are less clear. It is known that with sufficiently high MTX concentrations over time MTX is polyglutamated intracellularly.21,22 The polyglutamation process prohibits these MTX molecules from leaving the cell and increases their affinity for the target enzymes involved in reducing folates. MTX toxicity therefore is concentration and time dependent. The rate and extent at which glucarpidase reduces extracellular MTX levels compared with extracorporeal techniques preventing further polyglutamation might be its main advantage. Also, by reducing systemic MTX levels further precipitation in the renal tubules might be prevented. Glucarpidase, however, does not directly affect the intracellular concentration of MTX.
Because MTX and leucovorin compete for a common uptake path into the cell, proportionally higher concentrations of leucovorin are required to achieve rescue in the presence of MTX.1 Plasma MTX concentrations should always be monitored closely and leucovorin therapy intensified and continued until MTX serum levels have decreased to non-toxic levels and there are no signs of ongoing toxicity. Reducing extracellular MTX levels might enhance leucovorin uptake into the cell. However, leucovorin also competes with MTX as a substrate for glucarpidase, although with a lower affinity. This effect decreases the exposure to leucovorin for up to 26 hours after administration of glucarpidase. A reduction of the efficacy of leucovorin therapy by glucarpidase poses a serious risk. This concern was raised in the withdrawal report for glucarpidase at the European Medicines Agency (EMA).23
Given the lack of evidence of the effect of glucarpidase on intracellular levels of MTX and the possible negative effect it has on leucovorin rescue therapy, it is unfortunate that none of the case series compared the results of glucarpidase treatment to patients receiving standard supportive care in clinically relevant outcome parameters such as mortality or time to return to normal kidney function. In fact, despite glucarpidase treatment, mortality in one case series was as high as 23%.18 In our patient renal function returned to near baseline levels more than one month after glucarpidase therapy.
Glucarpidase is currently not registered on the European market and only available directly from the manufacturer. Orders are generally delivered within 24 hours within the Netherlands, but this still causes a delay in initiation of treatment.
At the time of application to the EMA, no dose-finding study had been performed to determine optimal dosage. A dose of 50 U/kg is recommended by the manufacturer; however, the proposed dose is not justified by clinical data and it is not shown that repeated use of glucarpidase is beneficial. Animal studies suggest that lower doses might have the same results.23 In two of the case series some patients received lower doses of glucarpidase. Unfortunately, the decrease in MTX levels was not reported separately for these patients.17,18 In a normal adult of 70 kg, treatment with 3500 units can cost up to 60,000 euro. A lower recommended dose could help to reduce the cost of treatment considerably.
CONCLUSION
MTX toxicity is a rare, but serious complication of high-dose MTX therapy. Supportive measures include first and foremost intensified leucovorin therapy together with hydration and urine alkalisation to maximise renal clearance. Glucarpidase is a relatively new agent that can rapidly and safely reduce extracellular MTX to non-toxic levels. However, glucarpidase does not reduce intracellular MTX levels and might reduce efficacy of leucovorin therapy. To date there is no randomised controlled trial comparing it with standard supportive measures on clinically relevant outcome parameters and treatment with glucarpidase carries a significant financial burden.
Because of these issues, we cannot recommend the use of glucarpidase in the treatment of MTX toxicity. There are no randomised clinical data to support the use in severe cases and theoretical evidence suggests that glucarpidase administration is unable to reverse high intracellular MTX concentrations after prolonged exposure to high MTX levels. Glucarpidase might be able to prevent irreversible MTX uptake into cells and limit direct effects of high MTX levels on kidney function. New randomised controlled studies should therefore be aimed at early administration of glucarpidase in patients with high levels shortly after administration of MTX. A recent meta-analysis of the observational data showed that administration of glucarpidase within 96 hours of MTX dosage reduced the development of severe toxicity.20 New studies should also include different treatment regimens for glucarpidase, since earlier studies suggest that a much lower dosage might be just as effective and could possibly reduce any deleterious side effects and cost of treatment.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES