KEYWORDS
Antimicrobial therapy, community-acquired pneumonia, guidelines
INTRODUCTION
Community-acquired pneumonia (CAP) is defined as an acute symptomatic infection of the lower respiratory tract in patients outside a hospital or a long-term care facility, whereby a new infiltrate is demonstrated.1,2 CAP is a common condition that carries a high burden of mortality and morbidity, particularly in the elderly.2,3 In the Netherlands, approximately 250,000 patients develop pneumonia each year (https://www.volksgezondheidenzorg.info, 2 August 2017). This translates into an incidence of 15 per 1000 person-years. Worldwide, CAP remains the second cause of death and life years lost.3
The Dutch Working Party on Antibiotic Policy (SWAB; Stichting Werkgroep Antibiotica Beleid), established by the Dutch Society for Infectious Diseases (VIZ), the Dutch Society for Medical Microbiology (NVMM) and the Dutch Society for Hospital Pharmacists (NVZA), coordinates activities in the Netherlands aimed at optimising antibiotic use, and containment of the development of antimicrobial resistance. In 2011 the SWAB and the Dutch Association of Chest Physicians (NVALT) published a joint guideline on the management of CAP. The present guideline is an update of this guideline, prepared by SWAB in collaboration with NVALT, the Dutch Society of Intensive Care (NVIC), and the Dutch College of General Practitioners (NHG).1 See textbox 1 for the methods.
Revision was considered necessary because in the past few years new – for a significant part Dutch – data have been published on the differences between the various disease severity classification systems on the percentage of patients treated as severe CAP, the sensitivity of chest computed tomography (CT scan) for diagnosis, the role of atypical coverage in patients with severe CAP, and the role of adjunctive prednisone therapy. Therefore, the Guideline committee decided to update the recommendations on imaging, empirical treatment, and the use of corticosteroids in CAP. It should be stressed that other parts of the guideline were not updated and show a large overlap with the previously published 2011 guideline.1 This is indicated for the relevant sections. See textbox 2 for a short summary of all the new recommendations compared with the 2011 guideline.
The CAP guideline focusses on the initial treatment of suspected CAP in adult patients who present to the hospital, and are treated as outpatients, and hospitalised patients up to 72 hours after admission. Pneumonia in immunocompromised patients is outside the scope of this guideline. 
CAUSATIVE BACTERIAL SPECIES OF CAP IN THE NETHERLANDS AND THEIR ANTIBIOTIC SUSCEPTIBILITY
Streptococcus pneumoniae remains the most commonly isolated bacterial pathogen causing CAP and should therefore always be covered in empirical treatment.1 The annual number of registered Legionella infections in the Netherlands is stable at around 300 cases per year (http://www.rivm.nl/Onderwerpen/L/Legionella). From 2007 to 2010 the Netherlands experienced a large Q fever outbreak, caused by Coxiella burnetii, leading to a large number of hospital admissions, mostly for CAP, in those years. No other major shifts in the aetiology of CAP were observed in the last five years, although it should be emphasised that in up to half of CAP episodes no causative microorganism can be identified (table 1).4-7 In patients with severe CAP and in patients who are admitted to the intensive care unit (ICU), Legionella spp., Staphylococcus aureus and Gram-negative infections are encountered more frequently compared with patients with mild to moderately severe CAP (table 1).4-7 Recent retrospective data points to the need for increased awareness of Aspergillus infection as a complication of H1N1 influenza A virus infection in critically ill patients on the ICU.8 It should be noted that the occurrence of atypical pathogens (Legionella spp., C. burnetii, Mycoplasma pneumoniae, and Chlamydia/Chlamydophila species) in patients admitted to the ward with a CURB-65 score of ≥ 3 is very low (table 1).9
The resistance percentage of S. pneumoniae for erythromycin is 12%, for co-trimoxazole 7% and for doxycycline 9%.10 Resistance to levofloxacin and moxifloxacin is very uncommon. In the Netherlands, high-level penicillin-resistant S. pneumoniae is extremely rare (< 1%) and thus does not require coverage by empirical antibiotic therapy. High-level resistance to penicillin should be considered in patients not – or insufficiently – responding to empirical treatment with penicillin or amoxicillin and with a recent travel history abroad. In such patients, increasing the dosage of penicillin or a switch to a cephalosporin should be considered.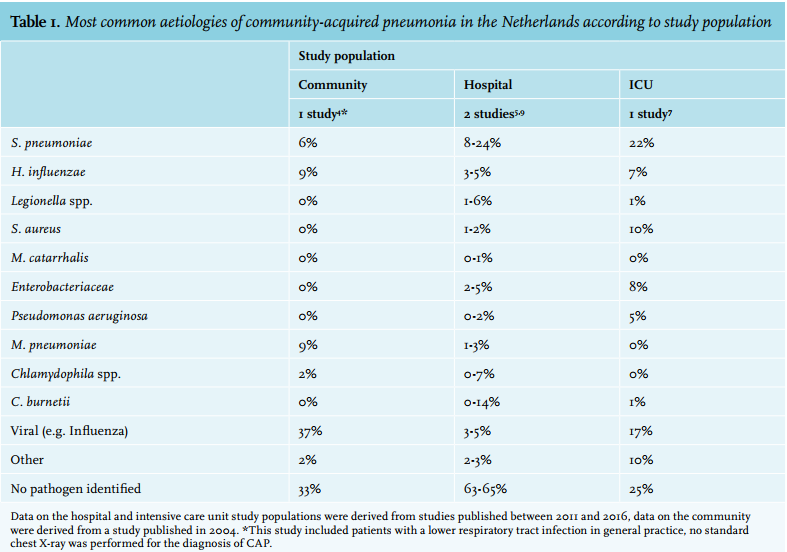
SEVERITY OF DISEASE UPON PRESENTATION IS USED FOR THE CHOICE OF INITIAL TREATMENT
Patients with CAP may be classified according to severity: mild, moderate-severe and severe CAP. Selection of empirical antibiotic therapy should be guided by the severity of the disease at presentation. Three scoring systems are in use. The Pneumonia Severity Index (PSI or Fine score) and the CURB-65 score (table 2) 1,11-13 are validated scoring systems, equally reliable in predicting 30-day mortality in patients hospitalised with CAP.14-16 Alternatively, a pragmatic classification (treatment at home; admission to a general medical ward and admission to an ICU) can be used. It should be noted that there can be marked differences in the categorisation of severity using these different scoring systems. For instance, a Dutch study among 1047 patients admitted with CAP showed that using a CURB-65 score > 2 as cut-off, almost twice as many patients were classified as having severe CAP as compared with the PSI score.17 However, with a cut-off CURB-65 score of > 3 less patients were classified as severe CAP compared with the PSI. As there is no gold standard, the committee does not recommend any of the scoring systems over the other; however, it is recommended that each hospital consistently uses only one of these scoring systems in daily practice. These recommendations are identical to the previous guideline.1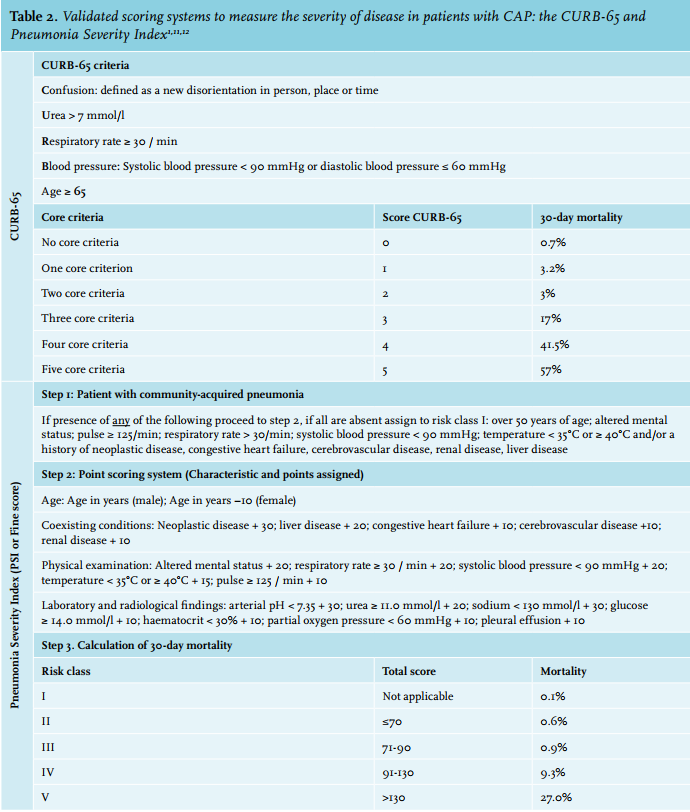
RADIOLOGICAL INVESTIGATIONS IN THE DIAGNOSTIC WORK-UP OF PATIENTS SUSPECTED FOR CAP
The chest X-ray does not allow prediction of the causative microorganism in CAP.18,19 The wider availability of low-dose CT scan facilities at emergency departments will likely lead to increased use of CT scanning of the chest in patients presenting with respiratory symptoms, and may ultimately replace the conventional chest X-ray. Recent data show that an early CT scan can improve diagnostic accuracy compared with chest X-ray.20 However, at present, there is not enough evidence to advocate the use of CT scanning as the new standard in patients evaluated for CAP. For patients with clinical features of CAP but without signs of infection on the initial chest X-ray, an additional chest X-ray within 48 hours may help to establish the diagnosis of CAP.21
MICROBIOLOGICAL INVESTIGATIONS
Although interpretation of Gram’s stain of sputum may allow early identification of the bacteriological cause of CAP, it is not recommended for guiding initial treatment. However, before starting antimicrobial therapy, blood and, if possible, sputum specimens should be obtained for culture, because culture results enable streamlining of antibiotic therapy and a switch to oral therapy if a specific pathogen is isolated. PCR results from nasopharyngeal swabs are considered the most reliable indicator for influenza virus replication in the human body.22,23 Validated PCR tests for respiratory viruses and atypical pathogens are preferred over serological tests. A urinary antigen test for Legionella spp. should be performed in all patients with severe CAP.24-27 One should, however, be aware that in the early stages of the disease the Legionella urinary antigen test may be falsely negative, especially in patients with mild pneumonia. In addition, with the current widely used test (immunochromatographic assay) only L. pneumophila type 1, which accounts for approximately 90% of Legionella cases, can be detected.
While the above recommendations have not changed compared with the previous guidelines,1 the usefulness of the urinary pneumococcal antigen test has been reconsidered. The sensitivity of the urinary pneumococcal antigen test for demonstrating a causative role of S. pneumonia in adult patients is low, but the test is highly specific.28-31 It has to be noted, however, that urinary pneumococcal antigens may be detectable in children, and also in adult patients with exacerbations of chronic obstructive pulmonary disease without pneumonia.32 It is now recommended to perform an urinary antigen test for S. pneumoniae in all patients treated for severe CAP. In patients with a positive test result and without another pathogen detected, antibiotic treatment can be simplified to amoxicillin or penicillin when the patient is treated on the ward. For patients on the ICU, therapy is de-escalated once clinical stability has been reached, which is often within 48 hours (figure 1).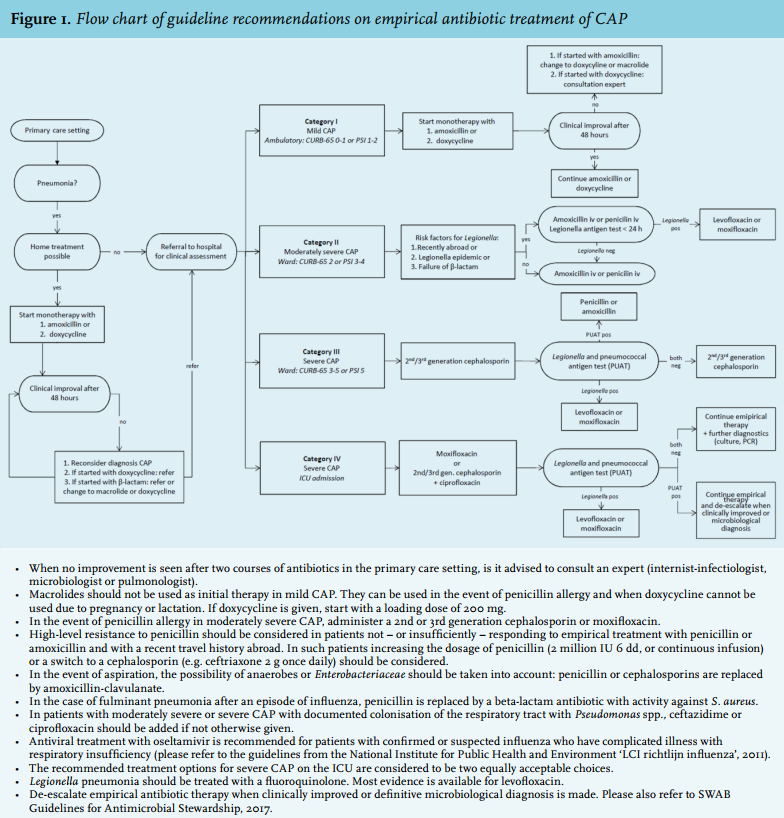
EMPIRICAL ANTIBIOTIC THERAPY FOR CAP
As compared with the previous guidelines, the most important change in the recommended empirical antibiotic therapy for CAP is to start with 2nd or 3rd generation cephalosporin monotherapy instead of combination therapy with amoxicillin or penicillin together with a quinolone or erythromycin in patients with severe CAP who are treated in a non-ICU ward. From an antibiotic stewardship perspective this is an important gain. The main reason for this change is the very low incidence of atypical pathogens in patients admitted to the ward with CURB-65 score ≥ 3 as outlined above. This is supported by the recent findings from the Dutch CAP-START study, involving more than 2000 patients with clinically suspected CAP admitted to non-ICU wards; in this study empirical treatment with beta-lactam monotherapy was non-inferior to strategies with a beta-lactam-macrolide combination or 4th generation f luoroquinolone monotherapy with regard to 90-day mortality.9 However, these data also indicated that Gram-negative bacteria and S. aureus are a more frequent cause of CAP among patients on the ward admitted with severe CAP when compared with patients with moderately severe CAP (CAP-START study, unpublished data) and, therefore, these pathogens should be covered in empirical therapy. Especially in patients with severe CAP, Legionella infection can be reliably ruled out with the urinary antigen test. To summarise, the recommendations for the empirical antibiotic therapy of the following four categories of CAP are as follows (table 3, figure 1):
Risk category I (mild CAP): CURB-65: 0-1, PSI: 1-2, non-hospitalised
For this group, initial therapy with a narrow spectrum beta-lactam antibiotic (1st choice) or doxycycline (2nd choice) is recommended. This is in accordance with the previous guidelines1 and the 2011 guidelines for patients treated by GPs.33 Doxycycline is not a first choice for this group in view of the 9% resistance of S. pneumoniae against doxycycline. The choice of a drug active against the most frequently occurring causative agent (S. pneumoniae) is essential in this case. Oral penicillin is not considered a first choice in view of the suboptimal gastrointestinal resorption. As a result of the increasing resistance of pneumococci against macrolides (10-14%), monotherapy with macrolides is discouraged unless the patient is allergic to penicillin and it is not possible to administer doxycycline (e.g. because of pregnancy or lactation). In that case, either clarithromycin or azithromycin are preferred. If there is a strong clinical suspicion of Legionella infection, then the Legionella urine antigen test must be carried out and empirical therapy must be adjusted. For patients in risk category I who receive amoxicillin or penicillin as initial therapy but do not improve within 48 hours, therapy should be switched to monotherapy with a macrolide or doxycycline. If therapy was initiated with doxycycline a switch to macrolides is not rational. In that case, referral to a hospital must be considered.1 In the outpatient setting, coverage for S. aureus in the influenza season, e.g. by amoxicillin-clavulanate, is not indicated.
Risk category II (moderate-severe CAP): CURB-65: 2, PSI: 3-4, admitted to non-ICU ward
For this category, initial therapy should be beta-lactam monotherapy, and the first choice is either intravenous penicillin or amoxicillin. Doxycycline and macrolides cannot be recommended because of the increasing pneumococcal resistance. Broad-spectrum antibiotics such as amoxicillin-clavulanate, cefuroxime, ceftriaxone or cefotaxime are not recommended because the expected pathogens do not justify the broader spectrum. In case of penicillin allergy, the best alternatives are a 2nd or 3rd generation cephalosporin or a 4th generation quinolone. If a patient of category II has one or more of the following risk factors for Legionella spp. a Legionella antigen test should be performed within 24 hours: 1) a recent visit to a foreign country, 2) coming from an epidemic setting of Legionella spp. infections, 3) failure to improve despite ≥ 48 hours of treatment with a beta-lactam antibiotic at an adequate dosage without evidence of abnormal absorption or non-compliance. If the Legionella antigen test is positive, therapy must be switched to monotherapy directed against Legionella spp. For Legionella pneumonia, levofloxacin has the most clinical evidence to support its use.
Risk category III (severe CAP): CURB-65: 3-5, PSI: 5, admitted to non-ICU ward
Therapy should be started with a 2nd or 3rd generation cephalosporin, because of the higher incidence of Gram-negative bacteria, and to a lesser extent S. aureus, in this patient group. For all patients in category III, a Legionella and pneumococcal urinary antigen test should be carried out as a routine procedure within 12-24 hours of admission. If the Legionella test is positive, monotherapy directed against Legionella spp. is recommended. If the pneumococcal urinary antigen test is positive, therapy can be narrowed to penicillin or amoxicillin. If both are negative, therapy should be continued with a 2nd or 3rd generation cephalosporin.
Risk category IV (severe CAP): admission to ICU
In this category, it is always recommended to cover S. pneumoniae, Legionella spp., S. aureus and Gram-negative bacteria. For this purpose there are two equally acceptable choices, both with excellent antimicrobial activity against all the expected causative agents. The choice is dependent, on the one hand, on the risk of development of antimicrobial resistance at the population level; on the other hand, the costs, the ease of administration and the profile of side effects play an important role:
• Monotherapy with moxifloxacin or
• Combination therapy with a 2nd or 3rd generation cephalosporin and ciprofloxacin.
Moxifloxacin is preferred over levofloxacin because of its high activity against pneumococci, favourable pharmacodynamic characteristics and good tissue penetration. Potential prolongation of the QT interval should be taken into account. Because of the high rate of side effects associated with their intravenous administration, macrolides are no longer recommended in this patient category.
For all patients in category IV, a Legionella urinary antigen and S. pneumoniae urine antigen test is carried out as a routine procedure within 12-24 hours of admission. If the Legionella test is positive, monotherapy directed against Legionella spp. is recommended. If the Legionella test is negative, the patient is still treated further with combination therapy (coverage of both S. pneumoniae and Legionella spp.) because the sensitivity of the urinary antigen test is not 100%. Since the specificity of the pneumococcal urine antigen test is < 100%, antibiotic treatment can be streamlined to penicillin or amoxicillin only in patients with a positive test result and without other pathogens detected if clinical stability (often within 48 hours) has been reached, or pneumococci have been cultured. In the event of a culture-proven causative agent, pathogen-directed antibiotic treatment is to be preferred at all times. 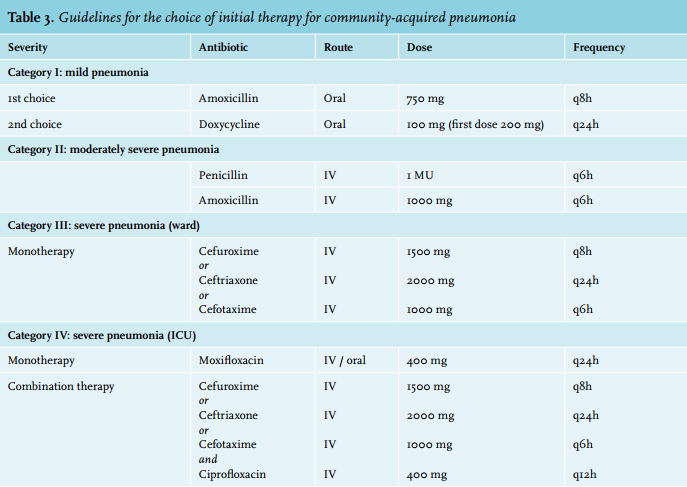
TIMING OF FIRST DOSE OF ANTIBIOTICS, TREATMENT DURATION AND SWITCH FROM INTRAVENOUS TO ORAL ROUTE
This section has not been altered compared with the 2011 guidelines.1 All patients should receive antibiotics as soon as the diagnosis of CAP is established. For patients with severe CAP admitted through the emergency department (ED), the first antibiotic dose should be administered within four hours of presentation and preferably while still in the ED. In patients with sepsis and septic shock, the recommendation of the Surviving Sepsis Campaign guidelines applies.34 Although the guidelines emphasise the importance of initiating antibiotic treatment rapidly, maximal efforts should be made to avoid inaccurate diagnosis of CAP and/or inappropriate utilisation of antibiotics.
If adult patients with mild to moderate-severe CAP are treated with a beta-lactam antibiotic or fluoroquinolones, the length of antibiotic treatment can be shortened to five days in those patients who have substantially improved after three days of treatment.35-37 Pneumonia caused by S. aureus should be treated for at least 14 days.25 Pneumonia caused by M. pneumoniae or Chlamydophila spp. is generally treated for 14 days,25 but no studies on treatment duration have been performed for these agents. For Legionella pneumonia a treatment duration of 7-10 days is sufficient in patients with a good clinical response.
Patients should be switched from intravenous to oral therapy when they have substantially improved clinically, have adequate oral intake and gastrointestinal absorption and are haemodynamically stable.38,39 For patients who fulfil these criteria, inpatient observation after switching to oral therapy is not needed.25,40
THE ROLE OF ADJUNCTIVE CORTICOSTEROIDS FOR PATIENTS WITH CAP
Over the last decade a whole range of potential immunomodulating therapies as adjunctive to antibiotics have been investigated in patients with CAP. Most data are available on the potential efficacy of corticosteroids. The three largest studies on adjunctive therapy with corticosteroids in patients with CAP5,41,42 yielded statistically significantly faster defervescence and, thereby, a shorter time to clinical stability and/or a shortening of length of hospital stay by one day for patients treated with corticosteroids. However, symptom resolution, overall cure rates, complication rates, ICU admission and mortality did not differ between patients with or without corticosteroid treatment. In all studies, the risk of hyperglycaemia was significantly higher in the corticosteroid-treated patients. In addition, treatment with short-term, high-dose corticosteroids may lead to other side effects, once applied routinely in larger populations. Therefore, the guidelines committee concluded, based on the available data, that the relatively small short-term benefits of adjunctive corticosteroids do not outweigh the potential disadvantages. As a result, the guidelines do not recommend corticosteroids as adjunctive therapy for treatment of CAP.
ACKNOWLEDGMENT
The Guidelines Committee would like to thank all individuals and societies who contributed to the development of these guidelines.
DISCLOSURES
Members of the preparatory committee reported the following potential conflicts of interest:
MJB: Novartis Europe advisory board Daptomycin, Pfizer Netherlands advisory board vaccines, grant from Pfizer Netherlands for investigating aetiology of CAP; WGB: received a grant from GSK and Astra Zeneca for research and a fee from Pfizer for medical advice; EMWG: grant from GSK for investigating aetiology of CAP; TJV: received two grants for research and a fee for consultation from Pfizer; APES: received support for conference attendance from Pfizer and AstraZeneca.
The other authors have no competing interests.
REFERENCES