ANSWER
The past medical history was suggestive for oral manifestation of a lymphoproliferative disorder, with the first hypothesis a deposit of amyloid.1 Plain macroglossia is a common sign of primary amyloidosis,1 while an increased volume with multiple nodules may be found in dialysis-related amyloidosis.2 In fact, macroglossia has been claimed to be a potential paraneoplastic sign of plasma cell dyscrasia. Nevertheless, in the present case bone marrow biopsy failed to identify any specific haematological disorder. When addressing other potential diagnoses, the absence of symptoms and the persistency of the relapsingremitting tongue swelling over several weeks lead to the exclusion of an acute inflammatory/infective disorder (e.g. tongue abscess). Other disorders to be excluded in case of relapsing-remitting tongue swelling over time were a false lingual artery, tuberculosis, syphilitic gumma, actinomycosis and infiltrating carcinoma.
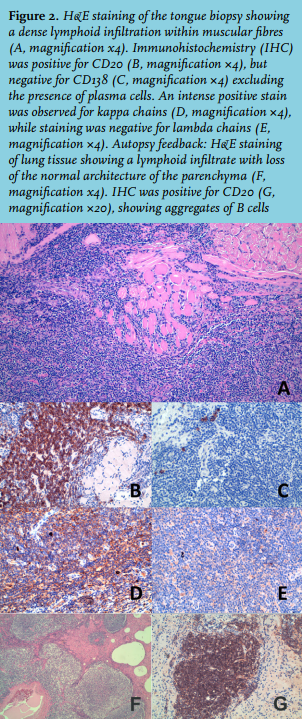
The pathological assessment of the oral biopsy showed mature B-cells (CD20+, CD3-, CD4-, CD5-, CD7-, CD8-, CD138-) with secretory capacity with stacks formed of kappa chains (figure 2). The joint assessment of such results, bone marrow biopsy and serum protein electrophoresis resulted in the diagnosis of Waldenstrom’s macroglobulinaemia with oral secondary manifestations. Two weeks after the diagnosis the patient died of a cardiac arrest. Death occurred because of direct damage to the heart and lung tissue due to massive deposition of M-protein and lymphocyte invasion, with a pathological appearance similar to what was observed in the tongue biopsy.
Oral manifestations of Waldenstrom’s macroglobulinaemia have been reported in just two patients, both of whom had gingival hyperplasia, in one case preceding the onset of massive oral ulcers.3,4
The present case reinforces the previously reported importance of an exhaustive assessment of macroglossia as a potential sign of haematological disorders.1
REFERENCES