KEYWORDS
Marjolin's ulcer, myositis ossificans traumatica, squamous cell carcinoma
INTRODUCTION
Myositis ossificans traumatica is a rare condition characterised by heterotopic bone formation of soft tissues. Based on clinical and histological data, the condition is often misdiagnosed as an infection or malignancy.1 However, a few cases of myositis ossificans traumatica transforming into a malignant tumour have been published.2,3 Ossifications by myositis ossificans traumatica may lead to cutaneous perforation accompanied by low-grade chronic infection with ulceration and sinus tracts. Chronic ulcers and wounds are known risk factors for the development of a type of squamous cell carcinoma called Marjolin’s ulcer.4 We describe a patient with myositis ossificans traumatica and a rapidly progressive and fatal course of metastatic squamous cell carcinoma primarily originating from a chronic ulcerated wound.
CASE REPORT
The patient, a 62-year-old woman, was admitted with general malaise, pain and swelling of the right leg. She had a known history of myositis ossificans traumatica since 1984 when she developed bilateral ossifications of the thighs, after removal of a lipoma from the right quadriceps region. Subsequently, she developed a chronic wound with multiple fistula on the right thigh which developed into a chronic and polymicrobial infection of the ossified muscles.5 Surgical debridement was not considered feasible as this would inevitably result in amputation of the right leg. With suppressive antibiotic therapy the infection remained controlled and she maintained functionality of her leg. Over the years, flares of infection were treated with antibiotics, mainly beta-lactam antibiotics, depending on cultures and antibiotic susceptibility.
In the last two months she had been suffering from general malaise and developed increasing pain, ulceration and swelling of her right thigh. On clinical examination the patient appeared weak. Examination of the right leg revealed an extensive, ulcerating and smelly wound with a diameter of approximately 20 cm (figure 1). On the medial side a large granulating, easily bleeding tumour of approximately 8 cm was visible. Laboratory investigations revealed hypercalcaemia of 3.36 mmol/l (2.15 to 2.55 mmol/l) and an increased parathyroid hormone-related peptide of 2.5 pmol/l (< 0.7 pmol/l). An ultrasound of the leg excluded deep vein thrombosis. A biopsy of the ulcerating tumour was performed and showed squamous cell carcinoma. A CT-thorax revealed multiple pulmonary nodules and two cavitating lesions in the left lower lobe and right upper lobe (figure 2).
A biopsy of one of the lung lesions was not conclusive. Cultures of the lung lesions were negative. An additional PET-CT showed enhanced metabolism of the right thigh, inguinal lymph nodes, para-aortic lymph nodes and bilateral, cavitating lung lesions (figure 3). Biopsies of inguinal lymph nodes were positive for metastatic squamous cell carcinoma. Additional immunohistological staining on biopsies of the right thigh and the inguinal lymph nodes showed the same p53 mutant pattern. Based on the long-lasting ulcerating wound, the locoregional metastatic pattern and the proven p53 mutations in both biopsies, we concluded that the metastatic squamous cell carcinoma most likely originated from the ulcerating tumour in her thigh. The patient was treated with bisphosphonates for her hypercalcaemia and started cetuximab for local control of the squamous cell carcinoma. Because of her clinical deterioration, palliative care was started and the patient was discharged to a hospice, where she passed away shortly after discharge.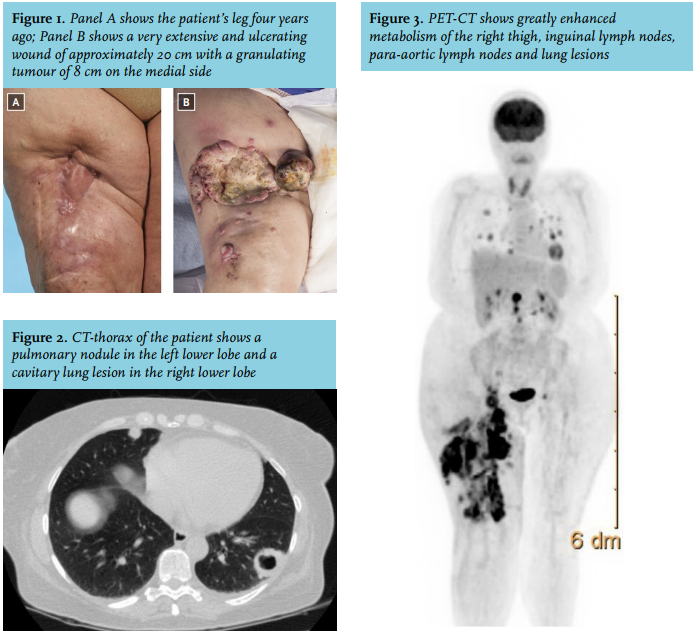
DISCUSSION
Myositis ossificans is characterised by heterotopic bone formation in soft tissues. Differentiating myositis ossificans from a soft tissue malignancy can be challenging and is based on clinical and pathological characteristics. Due to aggressive growth and pathological characteristics such as atypia and mitotic activity, myositis ossificans is sometimes misdiagnosed as malignancy, particularly osteosarcoma.1,6 Myositis ossificans can transform into osteosarcoma.2,3 Myositis ossificans can be divided into a progressive and a traumatic type. Progressive myositis ossificans (or Munchmeyer’s disease) is a congenital disease with autosomal dominant inheritance. Symptoms arise in early childhood; different muscles, tendons and ligaments may be affected. Traumatic myositis ossificans involves single muscles, muscle groups subjected to prior surgery or trauma and other soft tissues. Thigh and arm muscles are mostly affected, but also the hand, intercostal and jaw muscles can be affected.6-8 The exact mechanism for the pathogenesis of myositis ossificans traumatica is not clear. It has been suggested that trauma and intramuscular haemorrhage induce proliferation of vascular granulation tissue resulting in metaplasia to cartilaginous bone.8 Trauma induces a signal of bone morphogenetic protein, resulting in proliferation of mesenchymal cells to osteoblasts or chrondroblasts.9 Surgical treatment of the ossifications and affected muscles may be considered, but since repeated trauma can lead to new ossification this should be avoided as far as possible. Chronic ulcers, fistulas and wounds can transform into squamous cell carcinoma. Marjolin’s ulcer was first described in 1828 by Jean Nicholas Marjolin. In 1903 Da Costa reported malignant transformation of these ulcers.4 The incidence is low and represents about 2 to 5% of all squamous cell carcinomas of the skin.10 Transformation of a chronic wound or ulcer into a malignancy tends to be slow and develops over 20-35 years.11 Marjolin’s ulcers can be present anywhere on the skin but the trunk and extremities are particularly affected. The aetiology of the malignant transformation is not completely understood. It has been hypothesised that chronic wounds increase the likelihood of mutations. Due to fibrosis and avital tissue, circulating lymphocytes cannot reach and destroy the mutated cells resulting in impaired immunological activity.11 Marjolin’s ulcers have a high risk of recurrence and metastasising compared with other types of squamous cell carcinoma. Determining the primary site of metastatic squamous cell carcinoma by immunohistochemistry is generally not possible.12 The three-year survival for lymphogenic metastatic Marjolin’s ulcer is 35-50%.13 Patients with burn scars, chronic inflammatory dermatoses, ulcers, osteomyelitis and fistulas have an increased risk of transformation into squamous cell carcinoma.14 Physicians should be alert that patients with chronic wounds who develop increasing size, pain or bleeding tendency of the wound might have a malignant transformation and a biopsy might be warranted to exclude this potentially devastating condition.
CONCLUSION
To the best of our knowledge, we present for the first time a case of a rapid, progressive and fulminant course of metastatic squamous cell carcinoma arising from a chronic wound in a patient with myositis ossificans traumatica. Differentiating myositis ossificans from malignancy is challenging. In case of enlargement, pain, or bleeding tendency in patients with chronic fistulae, wounds and ulcers a histological biopsy should be considered.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES