DIAGNOSIS
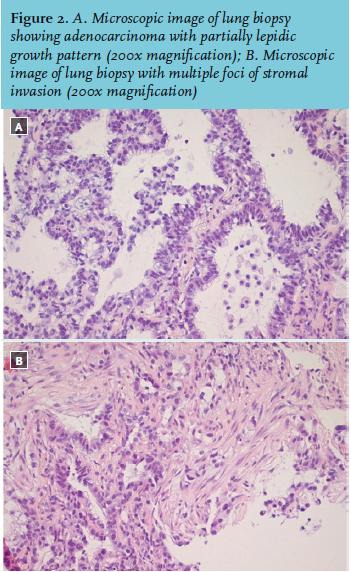
Ultimately transthoracic ultrasound guided 18 G needle biopsy was performed (figure 2), revealing a diagnosis and explanation why this patient did not improve despite full ICU treatment: lepidic predominant adenocarcinoma. Unfortunately there were no curative treatment options. Treatment was stopped and he died soon after. The family did not grant permission for autopsy.
Lepidic predominant adenocarcinoma (LPA), known as bronchioloalveolar carcinoma prior to the IASLC/ATS/ ERS lung adenocarcinoma classification from 2011,1,2 is often difficult to differentiate from pneumonia.3 LPA typically arises in the periphery of the lung, and grows along the alveolar walls, often without destruction of the underlying parenchyma.3 Because of this so called lepidic growth, radiographic images may be indistinguishable from pneumonia or can appear as ground glass opacity.2,3 Clinically, 62% of patients with LPA present without symptoms and with only an abnormal chest X-ray. The other 38% present with symptoms of cough, chest pain and sputum production, which in itself can lead to suspicion of infectious pneumonia. Bronchoscopic examination is usually normal.4 LPA may radiographically and clinically resemble not only pneumonia, but also non-infectious inflammatory processes (hypersensitivity pneumonitis, cryptogenic organising pneumonia, various vasculitic processes).3 Lack of fever and leucocytosis, with persistence of abnormal radiographic findings should raise suspicion about the correctness of a diagnosis of infectious pneumonia, and a focal or unilateral infiltrate points against many of the other non-malignant diseases mentioned above. Although hard to differentiate from infectious pneumonia, CT findings favouring the diagnosis of invasive adenocarcinoma include an air-filled bronchus within consolidation with stretching, squeezing, sweeping, widening of the branching angle and bulging of the inter-lobar fissure,5 coexisting nodules and a peripheral distribution of consolidation.6 An empirical trial of antibiotics and reassessment of clinical/radiographic findings is a reasonable approach. However, histological biopsy is the only means of diagnosing a malignancy and ruling out other aetiologies. Thus biopsy should always be considered when patients do not respond to antibiotics.3
DISCLOSURES
The authors have no conflicts of interest to declare.
REFERENCES