Full textPDF
Full text
CASE REPORT
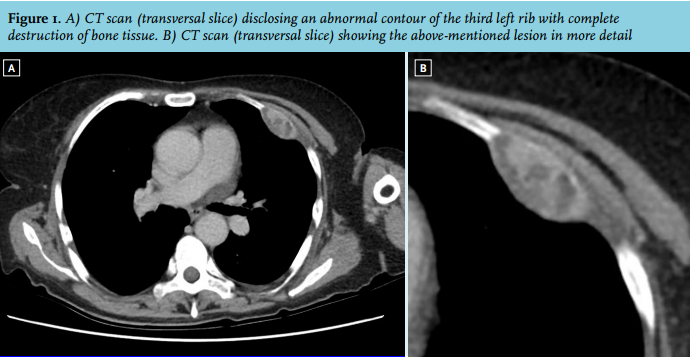
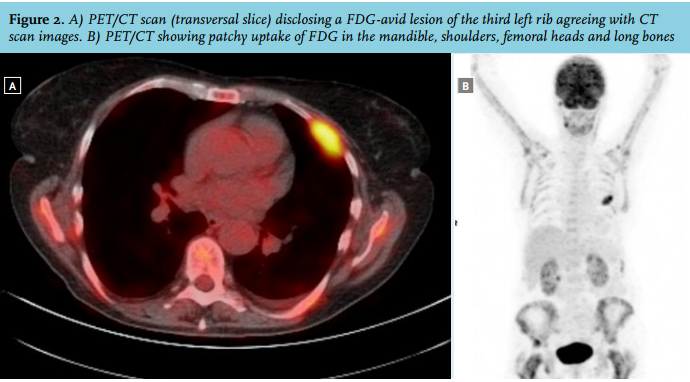
A 66-year-old woman was admitted to our hospital with a long-term history of bone pain, fatigue and myalgia. Some years earlier, she received radioactive iodine for toxic nodular struma followed by L-thyroxin substitution. At physical examination her thyroid gland was still enlarged. Laboratory data showed an elevated serum calcium level (4.16 mmol/l), alkaline phosphatase (767 U/l), parathyroid hormone (148 pmol/l) and low serum phosphate (0.83 mmol/l). CT scan showed left-sided multinodular enlargement of the thyroid gland and a bone lesion at the third rib but no enlargement of one or more parathyroid glands (figure 1A and B). Whilst the parathyroid hormone value was still unknown, the bone lesion seen on CT in combination with hypercalcaemia gave rise to the suspicion of malignancy. These findings prompted whole body positron emission tomography/ computed tomography (PET/ CT) to be able to image the whole skeleton and to differentiate avid from non-avid lesions. This study showed multiple FDG-avid osteolytic lesions in multiple ribs, the pelvis, scapulae, claviculae and femur, and humerus on both sides (figure 2A and B). In addition, to study the activity of the parathyroid glands a Tc-99m-sestamibi scan was performed. Intense uptake was found in the caudal region of the left thyroid lobe, with no retention in the skeletal lesions.
WHAT IS YOUR DIAGNOSIS?