DIAGNOSIS
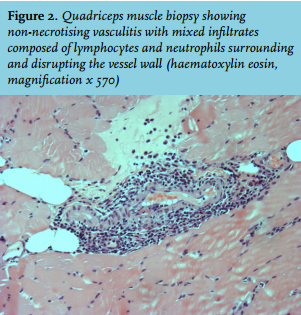
Muscle biopsy of the thigh revealed skeletal muscle non-necrotising vasculitis in the endomysium and perimysium tissue but no fibre necrosis or focal myophagocytosis (figure 2). Diagnosis of skeletal muscle vasculitis secondary to an acute PvB19 infection (that probably also presented in her son) was established. Of note, a viral infection was suggested because of the febrile eruption in her son, temperature and hepatitis. The patient declined treatment with intravenous immunoglobulins or glucocorticoids. Progressive resolution of pain and weakness was observed within two months under ketoprofen and the PvB19 PCR was negative four months later.
In patients with PSS, development of inflammatory myopathic conditions (polymyositis and dermatomyositis) is well known as well as vasculitis (mainly cutaneous vasculitis and mononeuritis multiplex), and in this latter case mainly associated with systemic disease activity of PSS and cryoglobulimaemia.1 Skeletal muscle vasculitis without any associated inflammatory myopathic conditions is rare. In a retrospective series including 40 patients with skeletal muscle vasculitis, clinical features consisted mainly of muscle pain, numbness in the extremities, fever, skin lesions and paresthesias, joint stiffness and pain.2 It has been described in association with rheumatoid arthritis, scleroderma, malignancies, and viral infections.2 Of note, two patients in this series had PSS.2 Histology revealed skeletal muscle necrosis, rarely non-necrotising vasculitis and neurogenic changes. Concomitant sural nerve biopsy showed nerve vasculitis and axonal loss. This nerve biopsy was not performed in our patient since the neurological examination and electromyogram were normal. Usually treatment relies on steroid therapy alone or associated with immunosuppressors.2
Acute PvB19 infections can develop in healthy adult patients but also in patients with hereditary haemolytic anaemia and underlying immunodeficiency. Besides cytopenia, clinical manifestations have been described including arthralgias, acute -rarely prolonged- symmetric arthritis, tenosynovitis, myocarditis, glomerulonephritis, encephalitis, exanthema, gloves-and-socks syndrome, hepatitis, rarely myositis and dermatomyositis,3 and cutaneous and skeletal muscle vasculitis including periarteritis nodosa.4 Administration of intravenous immunoglobulins is the first-line therapy, possibly in association with glucocorticoids.
Limb weakness and pain in a patient with PSS can indicate inflammatory myopathic conditions but also skeletal muscle vasculitis possibly related to acute PvB19 infection, as in our patient.
REFERENCES