KEYWORDS
Central venous catheter, (lung) ultrasound, chest X-ray, echocardiography, complications, general ward
INTRODUCTION
Patients on the general wards regularly need a central venous catheter (CVC) for the administration of intravenous feeds or medications, especially if a peripherally inserted central catheter is not feasible or for the purpose of haemodialysis.
Most CVCs, however, are introduced in the intensive care unit (ICU) or emergency department and it was estimated that in the UK 200,000 CVCs were inserted annually.1 For introduction of a CVC for patients on the general ward in our hospital, the patient has to be transported to a specialised unit or room and that will be the case in most other hospitals. If patients from the general ward are in need of a CVC, the use of ultrasound during and after insertion could be of great value. Using ultrasound during insertion will help in getting the CVC into the correct vessel, and because ultrasound can also be done immediately after insertion there will be no need to do a chest X-ray (CXR). This strategy might also be safe and time efficient for the general ward patients in need of a CVC.
It has been shown that the use of ultrasound during the insertion of a CVC in the internal jugular vein results in fewer complications and fewer attempts are necessary for correct placement compared with the landmark technique.2 Many guidelines and expert opinions prescribe the use of ultrasound guidance during insertion of a CVC into the internal jugular and subclavian vein.1,3-5
By using the Seldinger technique, a guide wire is introduced after puncture of the vessel under direct ultrasound guidance. Afterwards, the position of the wire is checked by ultrasound, further reducing the problem of misplacement.6 After introduction of a CVC, the position is checked by CXR, acknowledging that a pneumothorax or malposition may be missed through this investigation. Furthermore, there is little consensus on what the best position is on a chest radiograph;7 there are conflicting reports on the use of ultrasound for this question.8,9
Ultrasound has advantages compared with CXR.10,11 It has been shown to be superior to CXR in the identification of an anterior pneumothorax and can be performed immediately after the procedure, while waiting for a CXR takes time and is associated with discomfort and the need of radiation exposure for the patient. Furthermore, the immediate appearance of microbubbles in the right atrium after injection of agitated saline through the CVC proves unequivocally the intravascular position of the CVC.
We performed a proof of concept prospective study in which we compared ultrasound versus CXR in general ward patients receiving a CVC in the internal jugular or subclavian vein for the detection of post-insertion complications and to confirm the correct position of the CVC. Ultrasound was used as guidance during insertion. We also studied the time interval between the procedure itself and the results of the CXR.
MATERIAL AND METHODS
We conducted this study in a large teaching hospital in the Netherlands. General ward patients in need of a CVC were included. We excluded patients < 18 years and pregnant women. The study protocol was approved by the Local Ethics Committee and consent was obtained directly. Sex, age, body mass index, approach used for CVC placement, reason for CVC placement (antibiotics, total parental nutrition, lack of other venous access, combination of reasons) and the time (minutes) needed to obtain the result of a bedside CXR were noted.
Complications during insertion were noted separately (e.g. bleeding or rhythm disturbance).
All CVCs were placed under direct ultrasound guidance by experienced doctors (staff and residents). Due to logistic reasons general ward patients were transported to the ICU for insertion of the CVC during this study.
All CVCs were inserted using the Seldinger technique. After puncture of the vessel the position of the guide wire was checked by ultrasound in the long axis. In our departments triple lumen CVCs (Edwards Lifesciences) are used. For the left-sided CVCs a catheter of 20 cm is used, on the right side 15 cm. For dialysis purposes Medcomp catheters are used, also in two different lengths (20 and 15 cm).
After insertion, while waiting for the CXR, the following ultrasound examinations were performed by MB and FB, both experienced in the use of ultrasound:
Incorrect CVC position was defined as:
Position was defined as incorrect if there were no or few air bubbles, or a late appearance (> 2 seconds) of bubbles, seen from the superior vena cava entering the right atrium, or if there was turbulent flow in the right atrium or right ventricle.
The ultrasound examinations were done blinded from the CXR results. All CXRs were viewed by the attending radiologist who was not informed about the ultrasound results.
A true positive result was defined as the correct ultrasound placement confirmed by CXR and true negative placement as incorrect ultrasound confirmed by CXR. False positive was defined as correct placement by ultrasound not confirmed by CXR, and false negative placement as incorrect ultrasound placement not confirmed by CXR.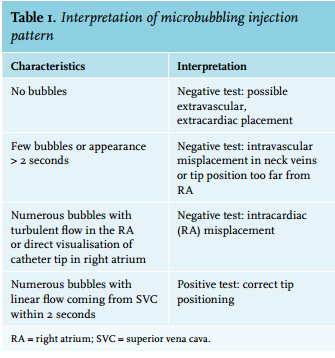
Calculation
Continuous data are presented as mean ± standard deviation (SD) or median and interquartile range (IQR) as appropriate. Categorical data are presented as frequencies and percentages. Using CXR as a reference standard, the sensitivity of ultrasound with a 95% confidence interval was calculated. Statistical analysis was performed using IBM SPSS Statistics (version 21).
RESULTS
Between January 2015 and September 2015, 53 patients were included (table 2). In this study 25 (47%) patients were male, aged 64 (± 12.8), with a body mass index (BMI) of 26.7 (± 5.2).
Other characteristics such as the reason for CVC insertion, the approach used (jugular or subclavian), whether the CVC was inserted by staff or a resident and the time needed for CVC insertion are also described in table 2.
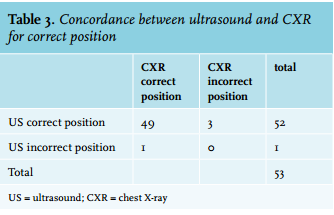
In all but one patient ultrasound was feasible. In one patient no cardiac view could be obtained. In one patient ultrasound revealed a correct position but the CXR showed an aberrant location of the catheter. In this patient the attending radiologist advised an iodine contrast cavogram which showed an anatomical anomaly of the superior vena cava. Therefore this CVC was correctly positioned in the superior vena cava. In one patient a catheter introduced in the internal jugular vein ended in the ipsilateral subclavian vein (also a large vessel). In this patient ultrasound showed a correct position, including normal pattern of microbubbles in the right atrium.
In one patient ultrasound showed a correct position but the radiologist concluded that the CVC was in the right atrium (table 3).
The sensitivity of the use of ultrasound in detecting that the CVC is correctly positioned (with CXR as a reference standard) was 98% (89.4-100%). The time needed for CVC placement was 17 ± 8.6 minutes (mean ± SD). The median time needed to wait for the result of the CXR was 24.5 minutes (IQR 18.1- 45.3). We omitted one patient who was included in the study when the digital radiology system was down for 44 hours due to severe technical failure.
In this study no post-procedural complications after CVC insertion were detected by either ultrasound and CXR.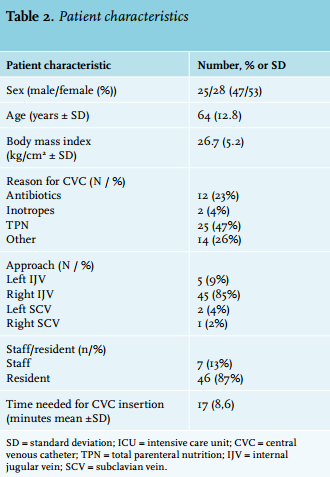
DISCUSSION
In this prospective observational study, we have shown that ultrasound is sufficient to exclude the existence of a pneumothorax and the absolute proof that the catheter is placed in a large vessel. For intensive care patients the use of ultrasound before and after CVC insertion has already been endorsed12 but ICU patients are not the only group of patients in need of a CVC. In this study we included general ward patients in need of a CVC. According to the current hospital protocol they were transported to the ICU for CVC insertion but this study opens the alternative of safely inserting a CVC in another designated area using mobile ultrasound. After insertion using ultrasound a check for correct positioning and complications can be done on the spot. In this way the patient is spared the burden of uncomfortable transport, extra waiting and additional radiation.
Furthermore, we have shown that a possible complication of the insertion can be examined immediately with ultrasound, while this is not the case with CXR. No post-insertion complications were found with either of these techniques. After insertion, ultrasound was directly used to check for position and complications. Extra time was needed to wait for the result of the CXR (median 24.5 minutes); in one case the result of the CXR was delayed for almost two days due to a serious technical failure.
In our study of 53 patients there were only three patients in whom discordance was found between ultrasound and CXR in determining the correct position of the CVC. In one patient the CXR proved to be wrong and in two patients ultrasound proved wrong (in one patient the radiologist found the CVC to be positioned in the right atrium which is a difficult call to make using bedside CXR). The position in the subclavian vein was of no clinical significance, since this is a large vessel, regularly used for access or for location of a peripherally inserted central catheter. The location in the right atrium was doubtful and probably also not significant. Comparing the two techniques, the sensitivity of the use of ultrasound in detecting whether the CVC was correctly positioned (with CXR as a reference standard) was 98% (90.1-100%).
There are more reports on the use of ultrasound after CVC insertion but these studies focus on ICU patients. There are more differences, for instance in our study we combined different factors to optimise correct positioning. All CVCs were inserted under direct ultrasound guidance including the identification of the guide wire before the skin; subcutaneous tissue and vessel wall were dilated. With the use of two different lengths (20 cm for left-sided lines and 15 cm for right-sided lines) the chance of a position being too deep in the average Dutch adult patient is limited.13,14
The use of different lengths is a different strategy compared with the study by Cortellaro et al.8 In the Cortellaro study CVCs of 20 cm length were used on both sides. They reported a very low incidence of incorrect positioning in the right atrium. Due to the fact that ultrasound identified only half of the incorrectly positioned CVCs, the authors state that ultrasound cannot substitute CXR in detecting incorrect positioning after insertion. In our study all but one of the CVCs were positioned above the right atrium and in almost all cases this was correctly detected by both CXR and ultrasound investigation.
In another study9 a good concordance between ultrasound and CXR was shown in detecting complications and correct position after CVC insertion. However, in this study ultrasound was not used as guidance during insertion. In this study also CVCs of 20 cm length were used on both sides and, compared with our study, substantially more subclavian veins were used (77% versus 5.7% in our study). In this study, due to the relatively high incidence of complications and incorrect positions of CVCs, good concordance between ultrasound and CXR in detecting complications and incorrect positioning was shown. In our study the a priori chance of complications and an incorrect position was limited by using ultrasound guidance during insertion and by using different catheter lengths for a leftand right-sided approach.
There is discussion about the correct position of CVCs anyway. In a recent review by Frykholm et al. the topic of catheter position was also discussed. After a search of the literature they concluded that there are no conclusive studies on optimal catheter tip position. Since less rigid catheter materials are used, the risk of cardiac tamponade associated with catheter tips in the right atrium is very low. In the case of a central line for the purpose of dialysis the position of the catheter tip in the right atrium might even be better.15
So perhaps the exact depth is less important than, for instance, whether the line follows the contour of the vessel (and is not perpendicular to the vessel wall).7 It is true that the angle of the CVC cannot be seen on ultrasound but in our study there were no cases of a CVC position perpendicular to the vessel wall and there is no scientific evidence that such a position might be dangerous. Furthermore, the rapid appearance of the contrast material in the right atrium proves a good flow of fluids through the catheter.
In a prospective clinical study by Pikwer et al.16 it was shown that when using CXR in 1619 patients there was a low incidence of detecting an incorrect CVC position. In only 0.37% the CVC position needed adjustment after insertion. They state that CXR should not be routinely used but only when the CVC insertion procedure was difficult. Another problem using CXR is that the CVC position may vary about 1 cm craniocaudally during breathing.17
In our study no complications were detected (0%). When introduced under direct ultrasound guidance, the incidence of complications after inserting a CVC in, for instance, the internal jugular vein is also reported to be very low.2,18 The sensitivity of lung ultrasound for the detection of pneumothorax is excellent when compared with CXR, which is known to be notorious for missing anterior pneumothorax.10,19
Another argument in favour of the use of ultrasound is the fact that ultrasound is more time efficient. In our study, due to technical failure the hospital radiology system (PACS) was out of order for 44 hours. Disregarding this incident, a substantial amount of time was needed before a CXR result was obtained. The time saving aspect can be of clinical significance.
Our study has a number of limitations. First, a small number of patients were included. The problem is that due to the a priori very low incidence of complications and incorrect positioning of CVCs the required number of inclusions is infeasibly high. Another criticism might be that in our study only doctors experienced in ultrasound were involved in performing the ultrasound examination after CVC insertion. Although with ample training point of care ultrasound can be taught20 it is possible that in less experienced hands the results would be different. The recognition of laminar versus turbulent flow in the right atrium requires experience but can also be taught when the right ultrasound view can be obtained.
Our patients had an average BMI of 26.7 (± 5). We did not select patients by BMI but included all possible patients so this set of patients represents the average Dutch patient in need of a CVC. The one patient in which no cardiac view could be obtained was a patient with a BMI of 28.7, who had undergone recent abdominal surgery. The low number of patients in which no cardiac view could be obtained in our study is not different from reports in recent literature.21
With modern ultrasound equipment adequate cardiac views can be obtained in the vast majority of patients.
CONCLUSION
Our proof of concept study shows that an integral use of ultrasound during and after CVC insertion is effective in establishing correct CVC positioning and post-procedural complications in patients from the general ward when compared with CXR. Our study demonstrates that CXR is only necessary if lung sliding cannot be demonstrated or if there is not a rapid (< 2 sec) appearance of microbubbles in the right atrium. To further investigate the occurrence of infrequently occurring complications, we suggest that a larger study should be performed.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES