KEYWORDS
Infectious diseases, haematopoietic stem cell recipients, viral infection
INTRODUCTION
Human metapneumovirus (hMPV) is an enveloped, single-stranded RNA virus that was first detected in 2001.1
However, according to serological studies the virus has already been circulating in humans for more than 50 years. It is a member of the Paramyxoviridae family, including respiratory syncytial virus (RSV) and parainfluenza virus. The virus contains eight genes, encoding nine proteins. Two of these proteins are the attachment protein G and the fusion protein F. There are four subtypes of hMPV: A1, A2, B1, B2, classified by the genotypes of the F and G proteins.2 Human MPV is distributed worldwide and thought to be transmitted by direct or close contact with contaminated secretions, such as saliva, droplets or large particle aerosols,3 with an incubation period estimated to be 4-6 days.4 Seroprevalence studies indicate that by the age of 5, most children have been infected with hMPV. In a retrospective study over a 25-year period, 20% of nasal-wash specimens from children with acute respiratory illness contained hMPV RNA.5 The mean age of infected children was 11.6 months. Human MPV appears second to RSV as a cause of lower respiratory tract infections in children.6 What seems less common is the attribution of hMPV to childhood upper airway infection (1 to 5%) which is lower than that observed for influenza, parainfluenza, adenovirus and RSV. In adults hMPV associated respiratory disease is also found. Human MPV was detected in 3.4% of adult patients with respiratory tract illness and can occur in adults of all ages.7 Several outbreaks of hMPV infections related to healthcare facilities have been described.8,9 Possible vectors of infection in these outbreaks were residents, as well as asymptomatic shedding of the virus in non-residents. Outbreaks were followed up by molecular subtyping of the virus in the respiratory specimen. Multiple subtypes can circulate at the same time and in the same location. Repeated infections are common.
The clinical symptoms of hMPV are similar to those of RSV and range from mild upper respiratory tract infection to severe pneumonia requiring mechanical ventilation, depending on age and health status of the host. Patients with haematological diseases, especially haematopoietic stem cell transplantation (HSCT) recipients are likely to be at increased risk of infection with a prolonged clinical course and risk of respiratory failure.10,11 We describe our experience with three HSCT patients diagnosed with respiratory infection with hMPV. These three patients were part of a much larger group of patients diagnosed with hMPV infection in that same time frame in our hospital (table 1).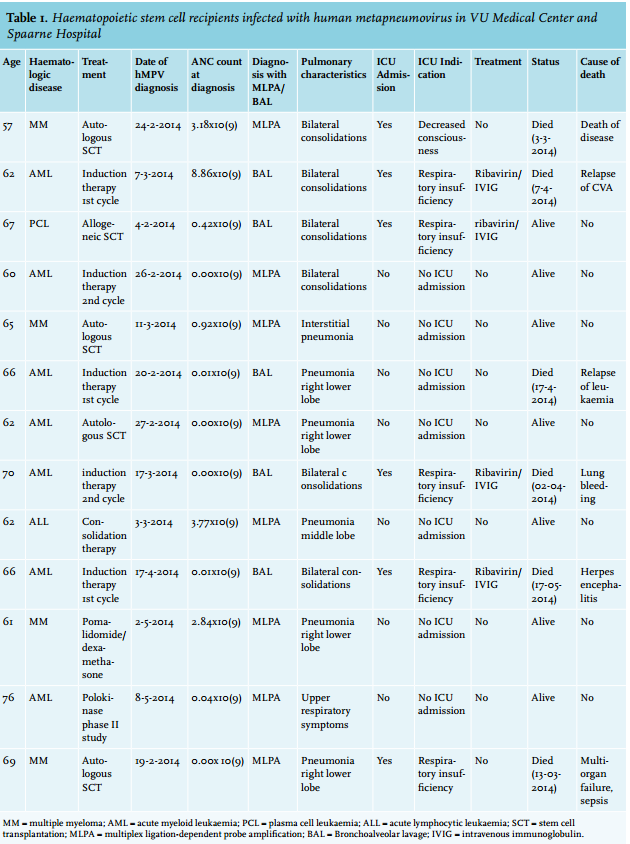
CASE 1
A 61-year-old male was diagnosed with acute myeloid leukaemia (monocytic, M5), with a good prognosis because of his NPM1 mutation status. He had no prior medical history, especially no respiratory conditions, and was a non-smoker. He was treated with two courses of induction chemotherapy and after the first cycle a complete remission was achieved. According to our national guidelines a third course of treatment was given, consisting of busulphan/ cyclophosphamide followed by autologous transplantation. Nine days after stem cell reinfusion, with an absolute neutrophil count of < 0.1 x 109/l, the patient developed fever and a dry cough. Lung auscultation revealed inspiratory crackles in the right lung and a chest X-ray showed signs of pneumonia in the right upper and lower lobe (figure 1). After performing sputum culture, blood cultures and a nasal swab for respiratory viral infections, treatment with the broad-spectrum antibiotic imipenem-cilastatin was started. The fever subsided but a non-productive cough persisted for over a week. After two days, multiplex ligation-dependent probe amplification (MLPA) of the throat showed a positive result for hMPV, while bacterial cultures of blood and sputum stayed negative. We decided not to start antiviral treatment because of the mild symptoms and signs of recovery. The clinical course was uneventful and the patient was discharged 17 days after stem cell reinfusion.
CASE 2
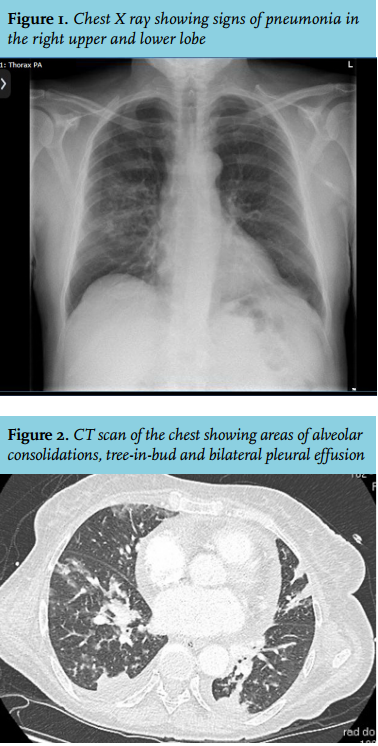
A 67-year-old female, with a history of asthmatic bronchitis, was diagnosed with plasma cell leukaemia in May 2013. She received four cycles of bortezomib, cyclophosphamide and dexamethasone and consolidation treatment with an autologous stem cell transplantation after high-dose melphalan. In January 2014 she was admitted for an allogenic stem cell transplantation with a sibling donor because of a poor cytogenetic risk profile. The conditioning regimen consisted of fludarabine, cyclophosphamide and total body irradiation (2 Gy), with cyclosporine A during a 30-day period after transplantation. Four days after transplantation, with an absolute neutrophil count of 0.42 x 109/l, the patient developed fever and dyspnoea. A computed tomography (CT) scan of the chest showed areas of alveolar consolidations, tree-in-bud and bilateral pleural effusion (figure 2). Under suspicion of bacterial pneumonia, imipenem-cilastatin was started. After three days, voriconazole was added because of persistent dyspnoea and fever. On day 8 after transplantation, her clinical condition worsened and the patient was transferred to the intensive care unit for respiratory support. Bronchial alveolar lavage was performed. MLPA showed a positive result for hMPV, other pathogens all tested negative. We started treatment with intravenous ribavirin with a loading dose of 30 mg/ kg followed by 16 mg/kg/day for four days and intravenous immunoglobulin 500 mg/kg for five days. One month after admission to the ICU she was successfully extubated and transferred to the haematology ward. Six months after the hMPV infection, she is recovering in a nursing facility, with up till now no signs of graft-versus-host disease or plasma cell leukaemia activity.
CASE 3
A 68-year-old man was diagnosed with progressive multiple myeloma. He received autologous stem cell transplantation in 2007 leading to complete remission. Further medical history included coronary artery disease. After six years of remission he developed progressive disease of his multiple myeloma for which he was treated with five cycles of velcade-dexamethasone followed by a second autologous stem cell transplantation after conditioning with high-dose melphalan. He developed fever, cold chills and non-productive cough the day before reinfusion of the stem cells, for which imipenemcilastatin was started. During stem cell reinfusion he developed an anaphylactic reaction, probably because of the dimethyl sulfoxide given with the cells, which was treated with clemastine and prednisolone. One day after stem cell transplantation he had progressive symptoms of non-productive cough, dyspnoea and fever. Lung auscultation revealed expiratory wheezing. Laboratory examination demonstrated an absolute neutrophil count of 0.1 x 109/l and chest X-ray showed a small infiltrate in the right upper lobe. Cultures of blood and sputum stayed negative. Because of persisting fever we added voriconazole empirically after three days. MLPA showed a positive result for hMPV, other respiratory pathogens all tested negative. Because of respiratory insufficiency the patient was admitted to the ICU. Intubation followed eight days after stem cell transplantation because of acute respiratory distress syndrome. A bronchial alveolar lavage was performed and hMPV still tested positive. No other pathogens could be demonstrated. Treatment was stopped on day 26 because of his progressive worsening condition and the patient died shortly afterwards.
IMMUNITY
The first line of defence in the lung is based on innate immune responses, activated upon recognition of a pathogen-associated molecular pattern by cell receptors on neutrophils, macrophages, natural killer cells and dendritic cells. These pathogen recognition receptors activate signalling pathways which leads to cytokine production and regulation of the inflammatory and immune responses in the infected host.10
The adaptive immune response (humoral and cellular) is the most important facet of protective immunity. Animal models have shown that passive transfer of antibodies protects from hMPV replication and have also demonstrated the essential role of T-lymphocytes in protection in hMPV infection. Recent observations indicate that CD8+ T cell response is impaired during hMPV infection.10 What is not clear is whether this defect is responsible for the commonly observed reinfections. Other studies suggest that repeated infections are likely due to waning immunity and limited cross-reactive antibodies.2
DIAGNOSIS
Patients with hMPV infection usually present with aspecific symptoms of a respiratory infection. The infection is associated with coughing, nasal congestion, dyspnoea, wheezing and fever. Older people (> 65 years) more frequently suffer from dyspnoea and wheezing than young people.13,14 More than 70% of virus infections occur in the winter months and over 80% of infections affect young children (< 5 years) or elderly patients. The virus can induce bronchitis, bronchiolitis and even pneumonitis. Pneumonitis is mainly seen in very young patients and patients with an immunosuppressive condition.14 In patients with haematological disease, stem cell recipients are at high risk to develop an infection. More than 40% of the stem cell recipients who develop hMPV infection also develop lower respiratory infection.15
Viral pneumonia is often not detected with conventional chest radiography. In patients with febrile neutropenia, 50% showed a pulmonary lesion on CT which was not detected with conventional radiography.16 Although different in type, viral infections have the same underlying pathogenic mechanism. Therefore, it is difficult to detect the type of viral agent with CT-based imaging. However, high-resolution CT of the chest is the technique with best discriminatory potential between different viral infections.16 In hMPV infections the most common findings are patchy areas of ground glass opacity, centrilobular nodules, bronchial wall thickening and multifocal areas of consolidation in a bilateral asymmetric distribution.16-19
Human MPV can be diagnosed most reliably by molecular techniques. In our laboratory, we use MLPA technology on nasopharyngeal swabs. MLPA uses a multiplex polymerase chain reaction method which can detect changes in the copy numbers of specific chromosomal regions of the virus.20 The sensitivity and specificity of MLPA to detect hMPV is high, 100% and 96% respectively.21,22 Haematological patients can suffer from various respiratory pathogens because of their immunosuppressed condition. With the technique of MLPA a number of respiratory pathogens including hMPV can be detected in one test run. The time to diagnosis is short for MLPA, as results can be available within six hours.23
TREATMENT
Few antiviral agents are available for treating paramyxovirus infections in general and treatment of hMPV infection is still mainly supportive. Although the natural course of this viral infection is associated with full recovery within 1-3 weeks, immunocompromised patients may benefit from early intervention.24
To date, experience has been gained from individual case reports and case series,25-27 with only ribavirin and immunoglobulins used in humans. Ribavirin inhibits RNA polymerase and demonstrated in vitro inhibition of tumour necrosis factor-alfa, interferon-gamma and interleukin-10.28 This suggests that ribavirin may influence and terminate T-cell immune-mediated damage caused by viral infections. Ribavirin can be administered intravenously, but aerosol therapy is also available. Aerosol ribavirin does have many disadvantages, because of its high cost and because it has direct teratogenic effects on healthcare workers. Especially healthcare providers who are pregnant or are attempting to become pregnant should avoid contact with patients receiving treatment with aerosolised ribavirin.29 Ribavirin in combination with intravenous immunoglobulin was reported to be effective in treating hMPV pneumonia in immunocompromised patients,30,31 but no randomised controlled trials in humans have been performed. Immunoglobulins for therapeutic goals can be divided into specific and non-specific immunoglobulin and currently human monoclonal antibodies with biological activity against hMPV are under investigation in vitro and in vivo.32 These new antibodies could be administered as a preventive measure but are also promising for use after infection. More innovative treatments concern the use of fusion inhibitors and RNA interference treatment modalities. Fusion inhibitors target the first steps of the viral replication cycle and are currently under investigation because of possible prophylactic use, particularly in post-exposure treatment of contacts of infected individuals.33 RNA interference depends on the action of small non-coding endogenous micro RNAs or exogenous small interfering RNA, which inhibit the translation of the mRNA or induce their cleavage, respectively. Several of these small interference RNAs were tested in vitro, and showed strong inhibitory activity.34 Another approach in the prevention or treatment of infection with hMPV is vaccine modalities. This is a challenging field because of the difficulty to induce a strong and long-lasting immune response, especially in immunocompromised individuals. Human MPV expresses the major surface glycoproteins F and H and immunisation strategies have been targeted against these surface proteins. Results of studies performed in rodent and non-human primate models look promising, with a variety of live-attenuated, virus vectored, inactivated virus and subunit vaccines.35 The primary strategy is to develop a live-attenuated virus for intranasal immunisation, generated by reverse genetics or recombinant proteins. The use of inactivated viruses for immunisation showed an enhanced immune response coupled to the absence of neutralising antibody production, which led to an increase in lung diseases in animal models. Research into inactivated vaccines for all paramyxoviruses has therefore been abandoned.36 Live attenuated vaccines also mimic natural infection, but have a considerably reduced ability to replicate, thus avoiding the development of disease.37
CONCLUSION
Human MPV is an important pathogen causing respiratory tract infections. Especially immunocompromised patients are at risk of developing severe respiratory complications, with considerable morbidity and mortality. Here we report three adult patients with hMPV infection after haematopoietic stem cell transplantation with a distinctly different disease course and outcome. While considerable progress has been made at the diagnostic level, proven treatment is still lacking. Ribavirin remains the only drug that has been used in humans to treat hMPV infection, but in the absence of randomised studies it is impossible to conclude with certainty on the efficacy of ribavirin. The development of a vaccine is desirable and ongoing studies are promising.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES