KEYWORDS
Hypocalcaemia, cancer, calcium metabolism, parathyroid hormone, critical care, rhabdomyolysis, tumour lysis syndrome, hypomagnesaemia, vitamin D, osteoblastic metastases.
INTRODUCTION
In patients with cancer, hypercalcaemia is common and may occur in up to 30%, often indicating advanced disease and poor prognosis.1 Lung, breast and haematological malignancies are involved in 84% of the cases but the mechanisms differ. Three major mechanisms have been identified: humoral hypercalcaemia due to secretion of parathyroid hormone (PTH)-related peptide by the tumour (for example, squamous cell carcinomas, renal, bladder, breast, or ovarian cancer), osteolytic bone lesions (for example, breast cancer or multiple myeloma), or production of 1,25-dihydroxyvitamin D (calcitriol) by the tumour (for example, lymphoma).2 In contrast, it is not well known that malignancy may also be associated with hypocalcaemia. A large variety of different and intriguing mechanisms may be involved and their full spectrum is not widely recognised.
Looking at these mechanisms, it might be conjectured that hypocalcaemia of malignancy will be increasingly encountered by clinicians in the future. We will present and discuss this entity in detail following the presentation of an exemplary patient. Our manuscript aims to draw attention to this potentially serious and relatively under-appreciated entity whose treatment is far from being uniform and must be adapted to its pathogenesis. It is based on a narrative review of the literature which covers incidence, pathogenetic mechanisms, aetiology-based diagnostic f lowchart, prognosis, and treatment recommendations.
CASE REPORT
A community-dwelling 89-year-old man was admitted with a few days history of cough, dyspnoea and refusal to eat. His past medical history included dementia and prostatitis identified in a biopsy performed five years previously for nocturia and a prostate specific antigen (PSA) level of 20 ng/ml (N < 4 ng/ml). He was not on any medications. On admission he was afebrile but hypoxaemic (saturation 91%), with bibasilar crepitations, elevated jugular venous pressure and leg oedema. A suprapubic prostatectomy scar was noted. ECG showed minor ST elevation in the precordial leads. Chest X-ray demonstrated pneumonia and pulmonary congestion. Blood test results are summarised in table 1. Six months before, the serum creatinine was 0.8 mg/dl, haemoglobin 10.8 g/dl and platelets 304 x 103/µl. Furosemide (80 mg), intravenous fluids (2.5 litres of saline), blood transfusions (2 units of packed cells) and antibiotics (ceftriaxone and azithromycin) were started. No hydronephrosis or masses were found on abdominal ultrasound. Urinalysis was unremarkable, sodium 10 mEq/l. The peripheral blood smear showed no fragmented erythrocytes. While the patient’s renal function improved to normal (creatinine 1.1 mg/dl) and the C-reactive protein significantly decreased, his hypocalcaemia unexpectedly worsened to 4.7 mg/dl with a serum albumin of 2 g/dl. Both were normal six months previously. The patient developed a positive Chvostek sign and prolonged QT interval. Serum phosphate, magnesium and creatine kinase were normal (table 1). The 25-hydroxyvitamin D level was 10.0 ng/ml (N > 50 ng/ml; < 8-10 identifies patients at high risk for osteomalacia). Intact parathyroid hormone (PTH) was increased to 319 pg/ml (N 15-68 pg/ml). Urinary 24-hour calcium level was 40 mg (N 100-300 mg). The prostatectomy pathology report arrived from another hospital, revealing that a markedly enlarged prostate (9 x 5.5 x 5 cm) resected four years ago had six foci of carcinoma involving the surgical margins, Gleason score 6. A bone scan was then normal and the patient declined treatment. A 99 mTc bone scintigraphy now revealed symmetric homogenous increased uptake in the skeleton, so called ‘super scan’ (figure 1), consistent with extensive bone metastases of prostate cancer.3 The current PSA returned markedly increased at 440 ng/ml. The hypocalcaemia was corrected by intravenous calcium gluconate (2 ampules of 10% solution equivalent to 180 mg elemental calcium in 50 ml 5% dextrose infused over 30 min and continued at 1.0 mg/ kg/h) plus oral calcium and calcitriol (0.25 μg, twice daily), but the patient died before oncological treatment could be commenced.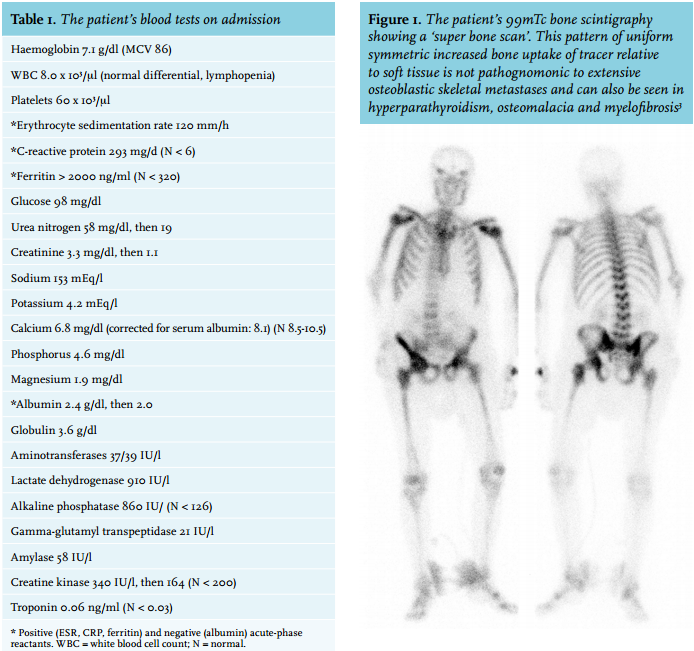
COMMENT
The patient presented with symptoms of congestive heart failure due to an acute myocardial infarction associated with pneumonia.4 We suspected the acute kidney injury and cytopenias were due to ADAMTS13 deficiency and thrombotic thrombocytopenic purpura, which can be triggered by infectious agents,5 but ruled it out. On admission, the hypocalcaemia (8.1 mg/dl, corrected for albumin) was considered incidental in an acutely ill geriatric patient with acute kidney injury. When he improved and the prerenal azotaemia resolved, his hypocalcaemia paradoxically worsened (6.3 mg/dl corrected for albumin). The differential diagnosis of hypocalcaemia in combination with elevated PTH and markedly increased alkaline phosphatase not related to the liver6 includes osteoblastic bone tumours and osteomalacia. Low urinary calcium excretion is common to both. Indeed, he had concomitant vitamin D deficiency – a common finding among cancer patients in correlation with disease stage7 and increasingly recognised in the general population.8,9 However, metabolic bone disease alone is unlikely to account for the extreme and escalating hypocalcaemia. Its unique pathogenesis in primarily osteoblastic metastases10,11 will be discussed below. Here, the presumptive diagnosis was supported by the associated marked cytopenias and confirmed by the pathology report, technetium bone scintigraphy and rising PSA levels.
METHODS
Most of the data on hypocalcaemia and cancer comes from case reports, case series or reviews of specific syndromes involving hypocalcaemia (e.g. tumour lysis syndrome, hypomagnesaemia, etc.). A narrative review methodology was therefore adopted. We searched PubMed using the terms cancer (or malignancy) and hypocalcaemia in adults, to capture and review all abstracted publications in the English language. Out of the abstracts (n = 777), more than 350 articles were reviewed. Any report of hypocalcaemia in the setting of cancer or its treatment was included, evaluated and classified according to the mechanism involved. A list comprising all the pathogenetic mechanisms identified was created. A few additional studies from the articles’ bibliographies were also included. Treatment recommendations were based on expert opinion and consensus statements, in the absence of more solid evidence.
Incidence of hypocalcaemia in malignancy
Only two studies have looked at the incidence of hypocalcaemia among cancer patients. Both are over 25 years old and their results are widely discrepant, probably due to differences in the patient populations studied. In Blomqvist’s study, 1.6% of 7625 ambulatory oncology patients were found to be hypocalcaemic,12 while D’Erasmo et al., who studied hospitalised patients, found an incidence of 10.8%.13 Since cancer treatment and survival has varied and several important aetiologies of hypocalcaemia in cancer may be more prevalent today, a current study is indicated, particularly among hospitalised patients. Thus, the entity seems to be far from rare. In patients with solid tumours and bone metastases, an incidence of 5-13% was reported by Riancho et al.14 and the difference depends on the formula used to correct total calcium for reduced serum albumin concentrations, which are common in cancer patients.15
Myriad of mechanisms of hypocalcaemia in malignancy
Hypocalcaemia, a decrease in extracellular calcium defined as serum total calcium < 8.5 mg/dl corrected for serum albumin, triggers an increase in PTH secretion to restore homeostasis by enhancing tubular calcium reabsorption in the kidney, stimulating osteoclastic bone resorption and promoting active vitamin D synthesis in the kidney (1,25-(OH)2D3, calcitriol), which increases intestinal calcium absorption and enhances PTH effects.2,16 Thus, hypocalcaemia develops when the net efflux of calcium from the extracellular fluid exceeds its replacement, due to disruption of these defence mechanisms such as occurs in reduced PTH or PTH resistance, vitamin D deficiency, or hyperphosphataemia secondary to decreased phosphate excretion or increased load.
Our literature review yielded altogether 12 potential mechanisms of hypocalcaemia in malignancy, excluding acute kidney injury /chronic kidney disease:
1. Pseudohypocalcaemia: in the context of hypoalbuminaemia (decreased binding) or recent MRI (gadolinium interference with assay). Ionised calcium remains unaffected but since hypoalbuminaemia is so common, its effect on serum total calcium must always be considered.
2. Calcium chelators: mild transient hypocalcaemia due to ionised calcium binding to citrate in patients receiving multiple transfusions.
3. Hypocalcaemia in the critically ill cancer patient (e.g. overwhelming infection, rapidly progressive disease): multiple mechanisms mediate hypocalcaemia,17 which may affect up to 70% of patients18 and be severe and ominous,19 possibly implicated in the development of critical illness polyneuromyopathy in ICU patients.20
4. Acute pancreatitis (e.g. secondary to hypercalcaemia of malignancy, drug therapies or the disease itself). Several incompletely understood mechanisms operate, predominantly precipitation of calcium soaps in the abdominal cavity.21,22
5. Acute hyperphosphataemia (leading to bone and extra-skeletal calcium-phosphate precipitation)
6. PTH deficiency: parathyroid gland destruction or removal: state after neck surgery for thyroid or laryngeal carcinoma (usually dissection, even minimally invasive), state after neck irradiation, rarely, parathyroid metastasis.11,27 Cinacalcet treatment (see below).
7. Magnesium depletion, causing PTH resistance (early) and decreased PTH secretion (late): chemotherapyinduced (e.g. cisplatin, cetuximab), antibiotic-induced (e.g. aminoglycosides, amphotericin), paraneoplastic renal magnesium losses (rare), post-obstructive diuresis, or protein-calorie malnutrition28 and poorly understood mechanisms (e.g. in cutaneous T-cell lymphoma).29
8. Ectopic calcitonin secretion by the tumour: other than medullary carcinoma of the thyroid (hypocalcaemia not reported), breast and lung carcinomas and hepatomas may produce calcitonin. Hypocalcaemia was very rarely reported,30 possibly associated with concurrent hypomagnesaemia.
9. Oncological drugs (other than those mentioned in #4, #5, #6, #7 and #10) often inhibiting osteoclastic bone resorption.31
10. Vitamin D deficiency: this exceedingly common condition9 is associated with age, malnutrition, staying indoors, hospitalisation, malabsorption, drugs that metabolise vitamin D (e.g. anticonvulsants), all common among cancer patients.7,16
11. Malabsorption: can occur in cancer patients either as a result of their specific disease (e.g. primary intestinal T cell lymphoma, enteropathy-associated or not; pancreatic exocrine insufficiency in pancreatic cancer)35 or develop in survivors, being related to their treatment (e.g. bacterial overgrowth after abdominal surgery, adverse effect of radiotherapy).36 In either case, hypocalcaemia is usually associated with low 25-hydroxyvitamin D and magnesium levels and malnutrition is a frequent contributing factor.
12. Osteoblastic metastases, with increased calcium uptake and utilisation:10 primarily carcinoma of the prostate or breast but also reported in gastrointestinal, lung, thyroid, salivary gland, and neuroendocrine cancer. In the rare osteosclerotic myeloma with or without POEMS syndrome, the same mechanism probably underlies hypocalcaemia.37
Commonly, more than one mechanism is operative, highlighting the need for a comprehensive evaluation of all the key ‘players’ to ensure successful treatment.
Aetiologies clarified and explained through a practical diagnostic workup
An informed use of a short set of clinical and laboratory data suffices for establishing the aetiological basis of hypocalcaemia in most cancer patients (figure 2). Such an understanding is imperative for treatment decisions.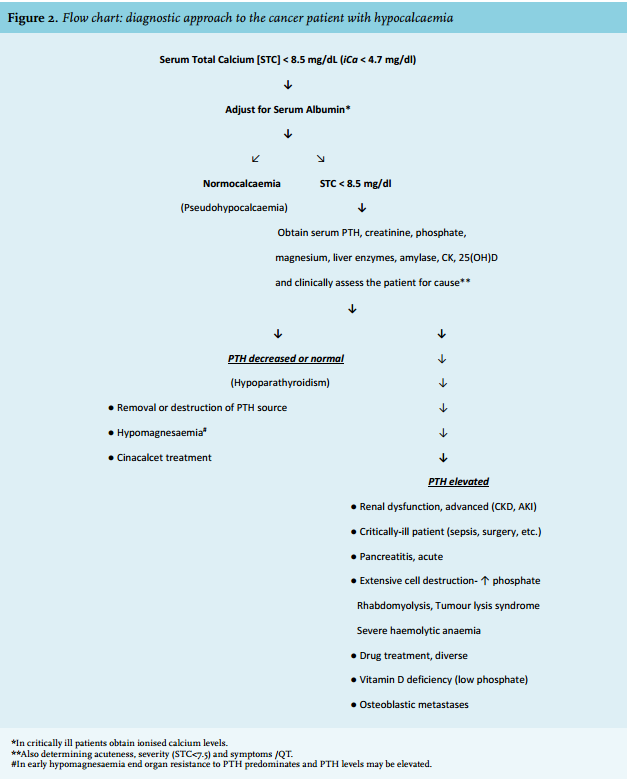
Phase 1. Confirm true hypocalcaemia. Since about half of the circulating calcium is bound to serum proteins (mostly albumin), hypoalbuminaemia, which is prevalent in cancer patients, will be associated with decreased serum total calcium but the clinically important ionised calcium fraction (iCa) remains unaffected. So-called ‘pseudohypocalcaemia’ is present when albumin-adjusted calcium levels are within the normal range (a convenient, commonly used formula is to add 0.8 mg/dl calcium for every g/l albumin below 4.0 g/l).15 In critically ill or post-surgical patients, it is better to obtain direct ionised calcium levels since binding is pH dependent.
Phase 2. Consider acuteness, severity and symptoms. Hypocalcaemia in cancer patients usually develops acutely or sub-acutely. Severity is defined as serum total calcium levels of less than 7.5 mg/dl (iCa < 4.0 mg/dl) and symptoms to look for are related to neuromuscular irritability. They include paraesthesias (circumoral or distal) and tetany, which may be overt (e.g. muscle cramps) or latent (Chvostek or Trousseau’s signs). At the serious side of the spectrum, laryngospasm, seizures, cardiac arrhythmias associated with prolongation of the QT interval in the ECG38 or vascular collapse may occur.
Phase 3. Assess prominent causes and obtain simple key tests. Although the next step in understanding the pathogenesis of hypocalcaemia is dependent upon determination of PTH status (figure 2),39 this may take time whereas basic clinical evaluation will often yield the likely cause. For example, Hastbacka and Pettila found hypocalcaemia in up to 85% of critically ill patients, including cancer patients.17 Multiple mechanisms had been implicated and in this setting ionised calcium should be measured: severe reductions (iCa < 4.0 mg/dl) seem to be an independent predictor of mortality in patients with severe acute kidney injury.19 The estimated glomerular filtration rate (eGFR) can be readily determined and advanced kidney dysfunction (late stage 4 and over, eGFR < 22 ml/ min/1.73m2 ) is a prominent cause of hypocalcaemia due to declining calcitriol levels and countering hyperphosphataemia by precipitation with calcium.40 Noticing a neck scar on examination or obtaining a history of neck surgery/irradiation suggests low PTH as the mechanism. Several ‘hypocalcaemic’ conditions can be readily diagnosed, such as acute pancreatitis whose hallmarks are pain, hyperamylasaemia and supportive imaging,21 rhabdomyolysis with marked increases in serum creatine kinase levels, hyperkalaemia, hyperphosphataemia and early hypocalcaemia due to calcium-phosphate deposition in necrotic muscle.41 Drug and chemotherapy history are of the utmost importance and may indicate tumour lysis syndrome, hypomagnesaemia or a specific drug effect (see under Mechanisms) as the likely cause.
Phase 4. Is PTH low (or normal, despite hypocalcaemia)? PTH is essential for calcium homeostasis and for maintaining normocalcaemia. However, the parathyroid glands may have been surgically removed due to cancer in the region (e.g. near-total thyroidectomy, common),42 irradiated, or rarely involved by metastases11 - easily identifiable conditions. Infiltration by iron following multiple transfusions (secondary haemochromatosis) has also been reported in cancer patients.43 Hypomagnesaemia (usually magnesium < 1.2 mg/dl) is commonly drug-induced (e.g. cisplatin, cetuximab)44 but may have many other varied causes in patients with malignancy,28 including a rare paraneoplastic tubular effect. Severe magnesium depletion markedly impairs PTH release in response to hypocalcaemia causing functional hypoparathyroidism, thereby also interfering with renal calcitriol production. Concurrently, PTH resistance develops, causing skeletal resistance and impaired PTH-induced calcium release from bone.27,45 Hypomagnesaemia is frequent in hospitalised patients. A study from the Mayo Clinic found a prevalence of 20.2% among 288,120 patients.46 Low levels were particularly common in haematology/oncology patients and often unrecognised unless specifically tested for. It is an important precursor of hypocalcaemia, found in 23.3% of patients with hypocalcaemia not due to renal failure.47 This hypocalcaemia is refractory to calcium but responds to continuous magnesium supplementation. Cinacalcet, a calcimimetic drug used in treating parathyroid carcinoma (or secondary hyperparathyroidism), inhibits PTH release and is another potential cause of ‘low-PTH hypocalcaemia’ in malignancy, which is usually asymptomatic and transient.48
Phase 5. Hypocalcaemia associated with elevated PTH concentrations. Otherwise, PTH is always increased in response to hypocalcaemia in an attempt at maintaining homeostasis. Malignant disease itself or its treatment can cause chronic kidney disease and acute kidney injury by a variety of prerenal, intrarenal (glomerular, tubulointerstitial, vascular) or postrenal mechanisms which often act concurrently and cause electrolyte abnormalities.49 With significant renal dysfunction and hyperphosphataemia,40 calcium-phosphate binding and precipitation cause hypocalcaemia. Thus, GFR and serum phosphate determinations are indispensable in evaluating hypocalcaemia. Exogenous administration of phosphate loads26 or extensive cell destruction23-25 releasing intracellular phosphate into the extracellular space during rhabdomyolysis, severe haemolysis or tumour lysis syndrome may also cause hypocalcaemia in cancer. With the emergence of new effective and targeted anticancer drugs, the incidence of tumour lysis syndrome is likely to rise.23,50 It is often associated with cytotoxic or monoclonal antibody treatment of haematological malignancies, but may also develop after radiation therapy, in treated solid tumours, and spontaneously.20 The greater the tumour burden and sensitivity to treatment, the greater the risk that massive tumour-cell lysis develops, releasing massive quantities of intracellular contents (potassium, phosphate, nucleic acids) into the systemic circulation and creating an oncological emergency. Acute kidney injury is central in tumour lysis syndrome and severe secondary hypocalcaemia to counter the phosphate load can be life-threatening and persistent.50 In rhabdomyolysis, when liberated phosphate from damaged muscle reaches critical levels in the serum, calcium-phosphate crystals form and are deposited in necrotic muscle.51 Hypocalcaemia in critically ill patients and in acute pancreatitis were discussed above. Importantly, hypocalcaemia is a recognised adverse reaction of multiple drugs used either in the treatment of cancer or its complications.31 Truly diverse mechanisms may be involved, as presented in detail above. They include drug-induced effects, tumour lysis syndrome, hypomagnesaemia, chelation, vitamin D deficiency, pancreatitis, drugs causing phosphate overload and inhibition of bone resorption. Each of these mechanisms is well supported by the literature, but some still remain poorly understood.32 The patient’s full drug history and awareness of these adverse drug reactions will establish the diagnosis.
Severe vitamin D deficiency (defined by serum 25-hydroxyvitamin D concentrations of < 20-25 nmol/l; hypocalcaemia is not usually observed above this level)39 is a major cause of hypocalcaemia, or a susceptibility to develop hypocalcaemia. Although not all these individuals develop overt osteomalacia, and retrospective case series show that serum calcium is often normal even in biopsy-proven nutritional osteomalacia,52 this cut-off is useful and identifies patients at high risk.9 Such ‘hypovitaminosis D’ is common among elderly patients and cancer patients in particular7 since they are likely to stay indoors without sun exposure (reducing cutaneous production) and suffer significant nutritional deficiencies (reducing intake). Commonly associated renal disease49 affects renal production of 1,25-dihydroxyvitamin D, or it may be malabsorbed or lost in cancer-associated nephrotic syndrome. As many as 74% of oncology outpatients in the study by Churilla et al. had low vitamin D levels,7 but a higher prevalence can be expected in the many patients who require hospitalisation.8 Nevertheless, in osteomalacia, serum calcium is reduced in about 1:3 patients only (while alkaline phosphatase increases are almost inevitable),52 and symptomatic hypocalcaemia is seen in ~10%. Severe reductions are particularly seen when a concurrent cause of hypocalcaemia coexists.
Avid calcium intake by extensive osteoblastic metastases (predominantly in prostate or breast cancer) is an intriguing cause of hypocalcaemia in cancer, which may rarely constitute its presenting feature.11 The mechanism of bone metastasis has been well studied: once within the bone microenvironment, prostate tumour cells proliferate, releasing multiple cytokines and growth factors which stimulate osteoblasts / stromal cells proliferation and production of further growth factors that also affect osteoclasts. A vicious cycle of tumour-cell growth and calcium-consuming new (but fragile) bone formation is propagated.53,54 This syndrome involves very common diseases which often metastasise to bone and therefore even low percentages translate into large numbers of patients. Among 155 patients with solid tumours metastatic to bone, up to 13% had hypocalcaemia and their metastases were almost exclusively osteoblastic.14 In stage M1 prostate cancer (spread beyond the lymph nodes), the prevalence of hypocalcaemia was double (27%). Tucci et al. studied a consecutive case series of 192 patients and reported 51 cases of albumin-corrected hypocalcaemia (26.6%), 125 patients with normocalcaemia and 16 (8.3%) had hypercalcaemia.56 While hypercalcaemia was associated with a poor prognosis (increased adverse skeletal events or death), hypocalcaemia was not. This finding was unexpected, especially since hypocalcaemic cases had a higher bone tumour load, but it was confirmed by Riancho et al.14 and Berruti et al. who consecutively enrolled 112 patients and concluded that hypocalcaemia was usually mild and asymptomatic.57 Despite an osteoblastic appearance on radiography, these metastases are also associated with increased osteoclast activity, providing the rational for treatment with osteoclast-targeted agents such as bisphosphonates or denosumab33 but also increasing the risk of significant hypocalcaemia.54,55
Lastly, finding one operative mechanism does not exclude the common existence of additional contributing ones. For example, hypoalbuminaemia and acute kidney injury may be found together with severe hypocalcaemia due to osteoblastic metastases and significant nutritional vitamin D deficiency, as in our patient; or as Bergkamp et al. eloquently demonstrate, an associated cancer or chemotherapy-related obtunded PTH response.58
Prognosis
Unlike hypercalcaemia of malignancy which is limited to three major mechanisms and its development is associated with poor prognosis,2 hypocalcaemia as a prognostic factor in cancer had never been studied systematically. However, its highly diverse mechanisms already suggest a more complex picture. Provided the patient is not critically ill,17 many cases of hypocalcaemia in cancer are relatively mild, asymptomatic and transient (e.g. most drug-related hypocalcaemia or hypovitaminosis D).31,52 The prognostic implications of hypocalcaemia in the setting of osteoblastic metastases have been discussed above56,57 and contrasted with hypercalcaemia.56 Hypocalcaemia can and should be anticipated in many of the more potentially significant and symptomatic syndromes (e.g. hypomagnesaemia, tumour lysis syndrome or bisphosphonate treatment) and can be reduced by monitoring before and during treatment and by the application of prophylactic measures as indicated (for example, among patients considered at risk of tumour lysis syndrome or magnesium depletion).50,59 Such measures may prevent some cases of hypocalcaemia or lead to their early detection and correction and to improvement in prognosis. However, symptomatic and even life-threatening hypocalcaemia in the context of cancer may still occur and mandate urgent treatment. Notwithstanding this variability, the underlying malignancy, its stage and amenability to treatment remain the cardinal prognostic factors in hypocalcaemia of malignancy.
Treatment
Treatment has also not been studied systematically, and recommendations are based on expert panel opinion, consensus statements and accepted practice or clinical experience, non-controlled trials or hard evidence. Generally, getting an early grasp on the pathogenesis (figure 2) is highly important, since calcium administration will hardly be effective unless essential deficiencies (for example, magnesium, vitamin D, or both) are attended to, and specific pathogenetic cascades mediating hypocalcaemia (for example, acute pancreatitis, tumour lysis syndrome or drug treatment) are targeted.50 Otherwise, treatment and monitoring does not differ from that of other settings of hypocalcaemia. The rate of decline, severity (usually serum total calcium < 7.5 mg/dl) and presence/severity of symptoms or QT prolongation (mild, severe, or life-threatening) determine treatment intensity. Several principles summarise the treatment of hypocalcaemia based on expert advice. First, the administration of calcium to severely hyperphosphataemic patients may result in widespread deleterious calciumphosphate deposition. Combined serum phosphate > 8 mg/ dl and symptomatic hypocalcaemia require dialysis to correct both. In asymptomatic patients, oral phosphate binders may improve hypocalcaemia too. Second, in symptomatic patients with associated hypomagnesaemia (< 1 mg/dl), intravenous magnesium sulphate (2 g in saline given over 30 min and followed by 4 g over 12 hrs) will allow correction of hypocalcaemia. Monitoring is required, particularly in patients with impaired renal function. Refractory unexplained hypocalcaemia in a susceptible patient may respond to magnesium even when normomagnesaemic.28 Third, in our experience, most patients will need concomitant vitamin D repletion (typically, 50,000 IU of vitamin D2 or D3 repeated as necessary). Finally, symptomatic / QT prolongation in hypocalcaemia patients (with neither hypomagnesaemia nor hyperphosphataemia) or patients with an acute decline < 7.5 mg/dl who will likely become symptomatic mandate intravenous calcium treatment. Calcium gluconate (1-2 g of 10% solution in 50 ml 5% dextrose given over 20 min, monitored and repeated) is an effective treatment.
CONCLUSIONS
With the advent of new potent drugs for the treatment of cancer and its skeletal complications, the increasing prevalence of vitamin D insufficiency and longer survival of patients with cancer, hypocalcaemia in malignancy is increasingly encountered in both hospitalised and ambulatory patients but nevertheless remains poorly recognised. A myriad of mechanisms may be involved, often concurrently, and they can often be evaluated almost instantaneously at the bedside. Their recognition and timely address may improve health outcomes and is of special importance in patients who may develop severe, even life-threatening symptoms.
DISCLOSURES
The author declares no conflict of interest. No funding or financial support was received.
REFERENCES