Full textPDF
Full text
CASE REPORT
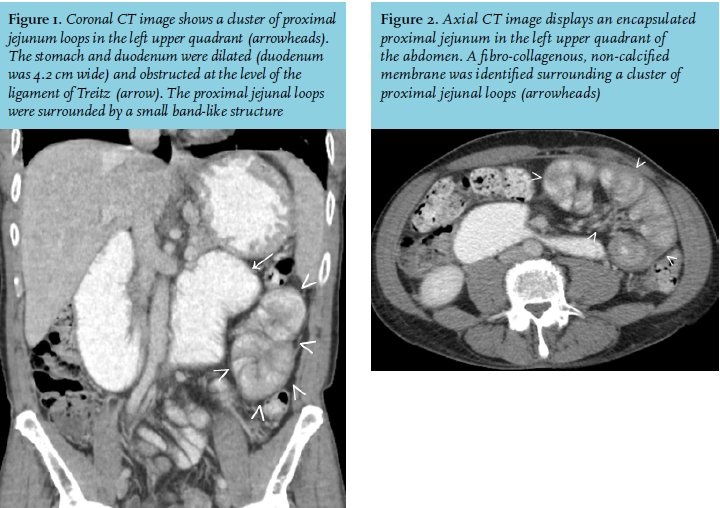
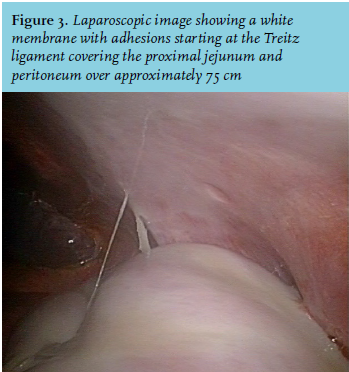
A 52-year-old man presented with a three-week history of abdominal pain, nausea and vomiting. His HIV-1 infection was successfully suppressed with antiretroviral therapy and in 2005 he was treated for pulmonary tuberculosis. At presentation in the emergency department he was haemodynamically stabile and physical examination showed no abnormalities. Laboratory results revealed mild signs of dehydration (blood urea nitrogen 7.9 mmol/l, creatinine 107 µmol/l, haematocrit 0.50 l/l) without signs of inflammation (C-reactive protein 3 mg/l). Abdominal ultrasound revealed multiple thickened, irregular small bowel loops. He was admitted to the internal medicine ward for rehydration and further evaluation. Because of persistent vomiting, a gastroduodenoscopy was performed. Stomach retention (without further abnormalities) was present despite the fact that the patient did not have any oral intake prior to the procedure. A CT scan of the abdomen showed a dilated stomach and duodenum up to 4.2 cm. There was a calibre change at the Treitz ligament with a subtotal obstruction of the jejunum. Furthermore, a fibro-collagenous, non-calcified membrane was surrounding a cluster of proximal jejunal loops (figure 1 and 2). In addition, a diagnostic laparoscopy was performed (figure 3).
WHAT IS YOUR DIAGNOSIS?