CASE REPORT
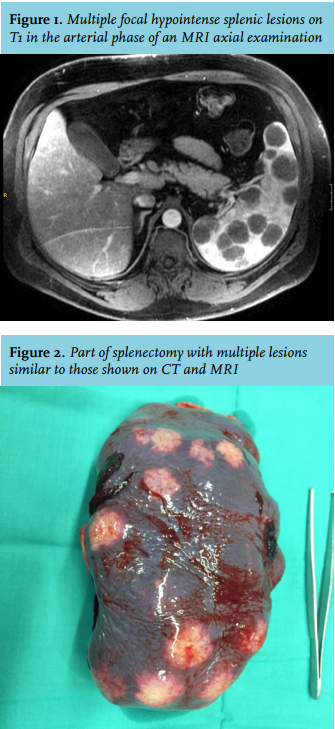
We present the case of a 43-year-old obese patient with type 2 diabetes. The abdominal ultrasonography performed in the context of an acute episode of renal colic showed multiple hypoechogenic hepatic lesions and an extended examination was required. A thoracic-abdominal CT scan was performed (figure 1) confirming the existence of multiple hepatic and splenic injuries and small thoracic and retroperitoneal lymphadenopathies.
Blood tests were performed and we found high levels of beta-2 microglobulin (> 3000 units), with all other results falling within the normal limits. The serology, autoantibodies, Mantoux and QuantiFERON tests were negative. A positron emission tomography was performed which showed lesions in the liver and spleen and multiple lymph nodes that had significantly increased fluordeoxyglucose uptake as compared to the surrounding parenchyma.
In order to reach a diagnosis, a splenectomy was scheduled. The result of the splenectomy (figure 2) was a piece of spleen of almost 900 g and 18 x 11 x 6.5 cm with multiple white superficial nodules, indurated, which represented 75% of the splenic parenchyma. On biopsy multiple granulomas of different sizes consisting of epithelioid cells, multinucleated Langerhans cells and small lymphocytes could be observed. It did not show necrosis. They were accompanied by vascular chronic inflammatory infiltrate. These findings were also present in ten lymph nodes in the splenic hilum. In addition, high levels of angiotensinconverting enzyme (132 U/l, normal range 13-64) were detected.
WHAT IS YOUR DIAGNOSIS?