KEYWORDS
Chronic lymphocytic leukaemia, comorbidity, spleen, radiotherapy, abscopal effect
INTRODUCTION
Chronic lymphocytic leukaemia (CLL), characterised by clonal proliferation and accumulation of mature B lymphocytes in blood, bone marrow, and lymphoid organs, is the most common type of leukaemia in the Western world.1 It mainly affects the elderly population, with a median age at diagnosis of about 70 years1. Many elderly CLL patients have comorbidities,2 which negatively impact survival.3,4 Treatment indications for CLL are well defined by international and national guidelines.5,6 Asymptomatic patients do not need treatment. For symptomatic patients, depending on age and clinical condition, there is a dichotomy in first-line therapy: go go for young and fit patients and slow go for older and less fit patients.5 For the young and fit patients the standard chemoimmunotherapy consists of fludarabine, cyclophosphamide, and rituximab (FCR), while for the less fit the standard therapy consists of chlorambucil monotherapy or in combination with rituximab.5,7 In addition to these traditional agents, many new and promising drugs directly targeting the B-cell receptor signalling pathway, such as ofatumumab, ibrutinib, idelalisib, and obinutuzumab, are about to be added, or are already added, to the therapeutic armamentarium.8-11 All these therapeutic options are palliative, and not curative. Because of severe comorbidities, sometimes even mild chemoimmunotherapy is not an option to palliate symptomatic, mostly elderly, patients.
An older palliative therapy of CLL is radiotherapy, which was the primary treatment of CLL before the introduction of modern chemotherapy,12 but which is no longer included in the current CLL treatment guidelines.5,6 Local radiotherapy can be employed when lymphadenopathy is bothering a patient, and splenic irradiation can be useful when patients experience symptoms related to splenomegaly.12
Here, we report the high prevalence of comorbidities in elderly patients with CLL as registered in the southern region of the population-based Netherlands Cancer Registry. We also describe the beneficial local and abscopal effects of splenic irradiation in four CLL patients, diagnosed and treated in a large non-academic teaching hospital in Delft, the Netherlands, who were unfit and/ or unwilling to undergo systemic therapy. In this exciting era for the treatment of CLL with many novel agents, we emphasise that the use of this old tool of splenic irradiation should not be forgotten as palliative treatment for elderly CLL patients with severe comorbidities.
METHODS
CLL patients registered at the Netherlands Cancer Registry
Clinical data of all cancer patients the Netherlands are registered at the Netherlands Cancer Registry, which is maintained by the Netherlands Comprehensive Cancer Organisation (IKNL). The Cancer Registry in the Eindhoven region records the data from all cancer patients in the southern Netherlands, an area with approximately 2.4 million inhabitants (about 15% of the Dutch population); there are no academic hospitals in this area. All patients diagnosed with CLL (ICD-O-3 code 9823) in the period 2002-2011, aged 35 and over, and recorded in the Eindhoven region of the Netherlands Cancer Registry, were included in this study. For the classification of comorbidity, a slight modification of the Charlson Comorbidity Index was used. Patients were arbitrarily divided into three age groups (35-59 years, 60-74 years, 75 years and over). A chi-square test was used to test for differences in the prevalence of comorbidity in the different age groups.
CLL patients undergoing splenic irradiation
Four consecutive, symptomatic CLL patients (three male, one female, age at diagnosis ranging from 65-77 years), diagnosed and treated in a large non-academic teaching hospital in Delft, the Netherlands, were unfit and/or unwilling to undergo systemic therapy, and were treated with splenic irradiation from 2012 onwards. Last follow-up was in April 2015.
Splenic irradiation
Whole-spleen irradiation was performed with a linear accelerator (6 MV) using anterior/posterior parallel opposing fields after CT planning. A total dose of 6 Gy, 12 x 0.5 Gy, twice weekly, was given to all patients. The total dose and fractionation schedule was based on previous studies on splenic irradiation in CLL, reviewed by Weinmann et al.12
Response criteria
CLL response criteria are defined by the International Workshop on Chronic Lymphocytic Leukaemia (IWCLL).13 Complete remission according to these criteria requires the absolute lymphocyte count to decrease < 4 x 109/l, ymph nodes to be < 1.5 cm, normalisation of liver and spleen size, constitutional symptoms to disappear, bone marrow to be free of CLL cells, and absolute neutrophil count to increase > 1.5 x 109/l, thrombocyte count > 100 x 109/l, and haemoglobin level > 6.8 mmol/l. In our patients, bone marrow biopsy was not performed after therapy for patient comfort and because of the absence of clinical consequences, and in most patients, a differential leukocyte count directly after therapy was not performed. Therefore, in our cohort, a complete response was defined when the leukocyte count normalised, thrombocyte count increased to > 100 x 109/l, haemoglobin level increased to > 6.8 mmol/l, and no hepatomegaly/splenomegaly and lymphadenopathy were detected on physical examination. Partial response was defined when the leukocyte count decreased by at least 50%, liver and spleen and enlarged lymph nodes decreased in size by at least 50% on physical examination, and thrombocyte count increased to > 100 x 109/l or haemoglobin level increased to > 6.8 mmol/l. Stable disease was defined when neither CLL remission nor progression occurred.
RESULTS
Elderly CLL patients frequently present with comorbid conditions
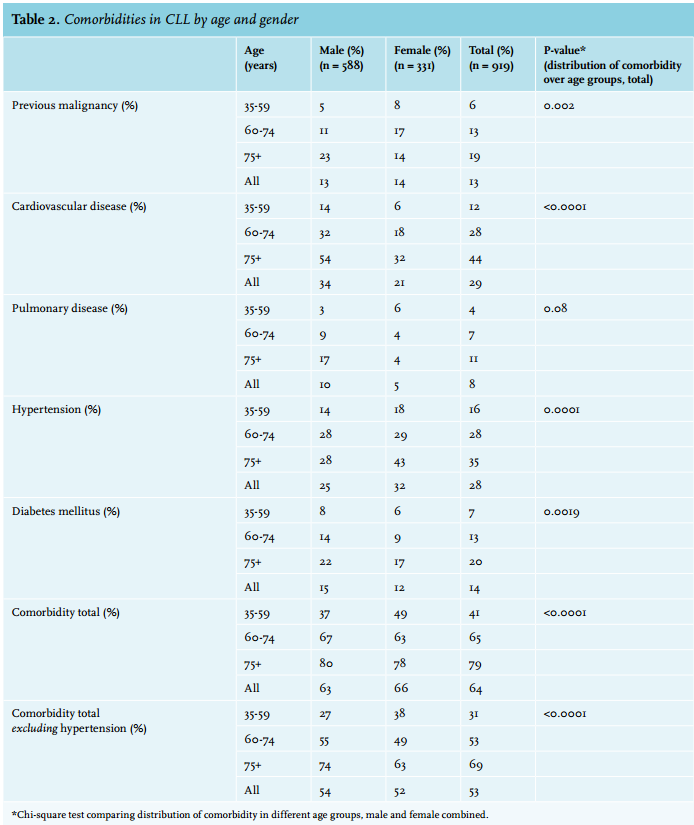
In the period 2002-2011, 919 CLL patients (588 male, 331 female) were registered in the Eindhoven region of the Netherlands Cancer Registry. The median age at diagnosis was 68 years (range, 36 to 97 years). Females were slightly older than males (median 71 vs. 67 years, respectively). Registered comorbid conditions were previous malignancies, cardiovascular disease, pulmonary disease, hypertension, and diabetes mellitus (table 1). In patients aged 60 to 75 years, one or more comorbidities were present in 67% of male patients, and in 63% of female patients. When hypertension was excluded, 55% of male patients, and 49% of female patients aged 60 to 75 years suffered from one or more comorbidities. The most frequently occurring comorbid condition in all age categories was cardiovascular disease (especially cardiac disease), which was present in 32% of male patients aged 60 to 75, and in 18% of female patients. Results are summarised in table 2.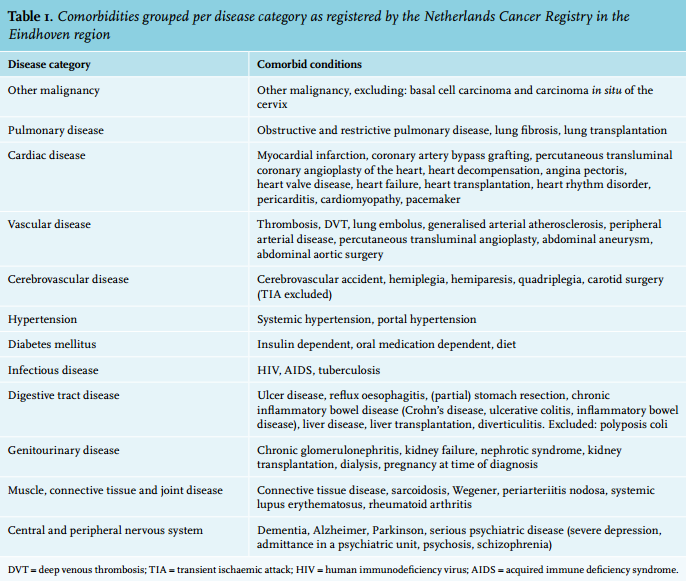
Splenic irradiation in symptomatic CLL patients has beneficial local and abscopal effects
Case A
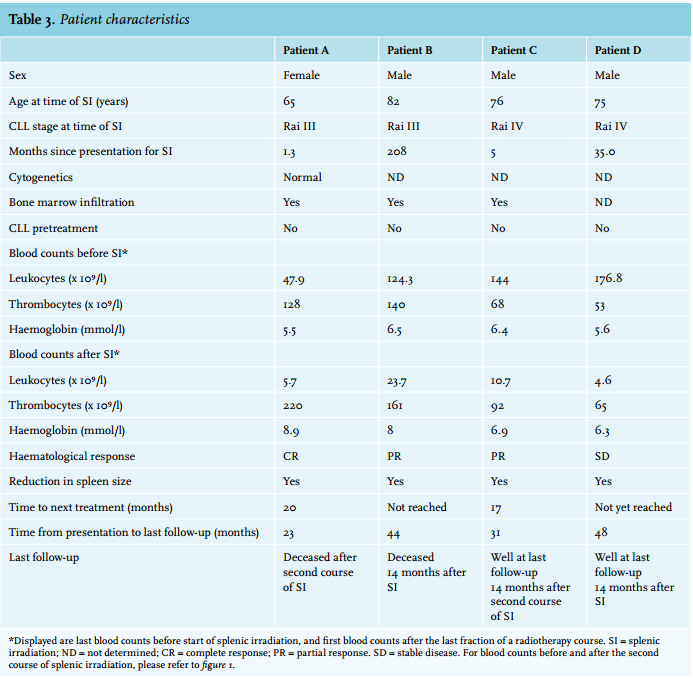
A then 65-year-old woman with a medical history of severe nicotine abuse and likely (although not documented) peripheral vascular disease, World Health Organisation (WHO) performance status 2, presented in 2012 with abdominal discomfort and tiredness. Physical examination revealed splenomegaly (19.4 x 7.4 cm by ultrasound) without lymphadenopathy, and laboratory results showed a leukocytosis of 54.8 x 109/l and atypical lymphocytes consisting of a monoclonal B-cell population. She was diagnosed with B-CLL/small lymphocytic lymphoma (SLL) RAI stage III. A bone marrow biopsy showed leukaemic cell bone marrow infiltration with replacement of normal haematopoiesis. Cytogenetic analysis was unremarkable. Because of splenomegaly causing mechanical complaints, the patient received splenic irradiation in 2012, in a total dose of 6 Gy (12 x 0.5 Gy, twice weekly). The patient’s spleen size normalised, lymph nodes remained undetectable, and a complete haematological response (based on normalisation of haemoglobin, thrombocyte and leukocyte levels) (figure 1A) with a very good clinical response was noted, without side effects. Two years later, in 2014, the patient again complained of tiredness, dyspnoea, and night sweats. Her splenomegaly had reappeared, blood counts had dropped, and her leukocyte count increased to 115.0 x 109/l. She received a second course of splenic irradiation (12 x 0.5 Gy, twice weekly), after which her spleen size normalised rapidly, her leukocyte count dropped, and peripheral blood counts increased (figure 1A). Unfortunately, about ten days after radiotherapy had started, the patient died due to complications of massive cerebral infarction. Thrombocyte count two days prior to the infarction was 237 x 109/l. It seems unlikely that the infarction is directly related to the splenic irradiation.
Case B
A then 65-year-old man, with a medical history of severe chronic obstructive pulmonary disease, was diagnosed with B-CLL RAI stage 0 in 1996. A bone marrow aspirate showed infiltration of bone marrow with CLL cells. The patient was asymptomatic, and a watch-and-wait policy was followed. The patient withdrew from follow-up from 2010 to 2013, but was recently admitted again to our hospital with a lower airway infection. Despite adequate treatment of the airway infection his condition remained fragile, with a WHO performance status 4. He complained of invalidating night sweats, discomfort in the upper abdomen, and weight loss. Furthermore, he remained dyspnoeic, and had hepatosplenomegaly (craniocaudal size of liver 17.5 cm, spleen size 15.6 x 15.6 cm by CT scan) and lymphadenopathy on physical examination. His laboratory results showed a leukocytosis of 124.3 x 109/l, anaemia and thrombocytopenia. A CT scan showed bilateral pulmonary consolidations, bullous emphysema, mediastinal, axillar and para-aortic lymphadenopathy, and a severe hepatosplenomegaly. Due to his frail condition, systemic chemotherapy, and even mild immunotherapy, were not options to treat his CLL-related symptoms. Because his splenomegaly caused abdominal discomfort and also compromised his pulmonary function, palliative splenic irradiation was given (12 x 0.5 Gy, twice weekly). After splenic irradiation, his clinical condition improved dramatically: night sweats and abdominal discomfort disappeared, his dyspnoea diminished, and on physical examination, the hepatosplenomegaly and lymphadenopathy disappeared. A partial haematological response was reached: his leukocyte count decreased, and haemoglobin and thrombocyte levels normalised (figure 1B). No significant side effects of splenic irradiation were noted. The patient was seen several times afterwards at our outpatient department with a markedly improved condition and without splenomegaly or lymphadenopathy. Unfortunately, 14 months after radiotherapy, the patient died unexpectedly at home, possibly due to pneumonia or pulmonary bleeding. At that time, his thrombocyte count and haemoglobin levels were normal, although his leukocyte count was slowly rising again.
Case C
A then 76-year-old man, with a medical history of low-risk prostate carcinoma, was diagnosed with symptomatic B-CLL RAI stage IV in 2012. At presentation, he was extremely tired, and he complained of discomfort in the upper abdomen. On physical examination, splenomegaly (19 x 8 cm by CT scan) was noted without lymphadenopathy. His leukocyte count was 79.9 x 109/l, and he was anaemic and thrombocytopenic. A bone marrow biopsy showed CLL bone marrow infiltration with significant replacement of normal haematopoiesis. Shortly after diagnosis, because of his symptomatic splenomegaly, palliative fractionated splenic irradiation was given (12 x 0.5 Gy, twice weekly). Hereafter, on physical examination, his spleen size decreased, lymph nodes remained undetectable, his clinical condition improved, and he showed a very good partial haematological response, based on haemoglobin, thrombocyte and leukocyte levels (figure 1C). No significant side effects were noted. One year later, the patient became tired again, his splenomegaly reappeared, while no lymphadenopathy was noted, and his leukocyte count increased to 122.9 x 109/l. The patient chose to undergo splenic irradiation again, with similar beneficial effects to his first course of radiotherapy. At the last follow-up, 14 months after the second round of splenic irradiation, the patient was well and asymptomatic.
Case D
A then 72-year-old man was diagnosed with asymptomatic B-CLL RAI stage 0 in 2010. His medical history consisted of prostate hypertrophy and renal insufficiency. In 2012, based on thrombocytopenia, his CLL progressed to an asymptomatic RAI stage IV, and a year later, he became symptomatic because of massive splenomegaly (spleen size one year earlier by ultrasound 17.5 x 8.4 cm). No lymphadenopathy was noted on physical examination. His leukocyte count had increased to 176.8 x 109/l. Bone marrow biopsy was not performed. The patient refused therapy with chlorambucil and/or rituximab, and splenic irradiation was started (12 x 0.5 Gy, twice weekly). No significant side effects were noted. Hereafter, his clinical condition improved greatly, his splenomegaly disappeared, lymph nodes remained undetectable, and his blood counts improved, although partial response criteria were not met (figure 1D). The patient is well at last follow-up, approximately 14 months after start of radiotherapy. The patient characteristics are summarised in table 3.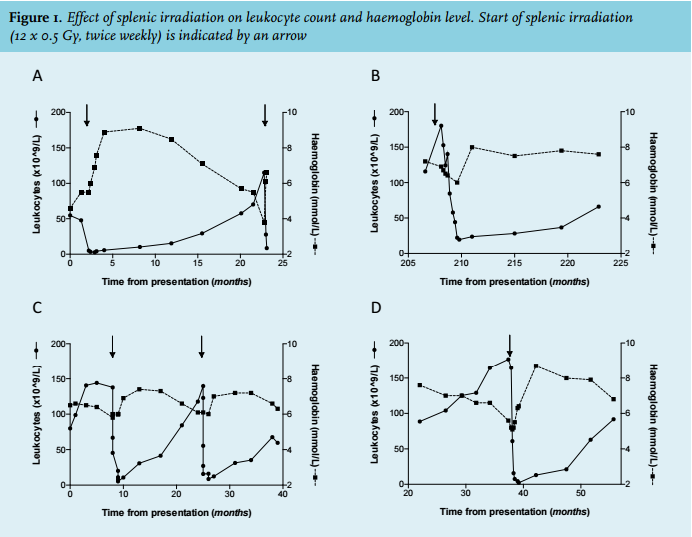
DISCUSSION
CLL is a malignancy that frequently occurs in elderly patients, who often have comorbidities. In a large prospective population-based cohort of 919 CLL patients, we report that more than half of the patients had one or more comorbid conditions. This is in line with the previously published frequency of 46% of newly diagnosed CLL patients with one or more major comorbidities (coronary artery disease, peripheral vascular disease, cerebrovascular disease, other cardiac disease, diabetes mellitus, COPD/respiratory disease or second malignancy, excluding non-melanomatous skin cancer).2
Due to these frequently occurring comorbidities, the use of old and novel chemoimmunotherapy regimens is frequently not feasible or refused by the patient. We show in four elderly symptomatic CLL patients who were unfit or unwilling to undergo systemic treatment that splenic irradiation is a very effective palliative treatment. Apart from effectively treating splenomegaly, these patients also obtained complete or partial haematological responses of significant duration.
Total body, total lymph node, mediastinal, or extracorporal irradiation have historically been used as primary treatment of CLL, but resulted in significant haematological and infectious complications. After the introduction of modern chemotherapy, it was demonstrated that these radiotherapy regimens had no superior effect compared with chemotherapy (reviewed by Paule et al.14). In contrast, in several historic studies, splenic irradiation was shown to not only be effective in resolving splenomegaly-related symptoms, but also to result in haematological responses with few side effects (reviewed by Weinmann et al.).12,15-20 The only larger historic trials directly comparing splenic irradiation with chemotherapy, the Medical Research Council (MRC) 1 and 2 trials, showed a similar survival in patients treated with splenic irradiation and those treated with chlorambucil.21 How exactly splenic irradiation exerts its beneficial effect in CLL is incompletely understood. Likely, there is a direct effect of irradiation by inducing apoptosis of malignant B lymphocytes (which are, like normal B lymphocytes, more radiosensitive than normal T lymphocytes) in the spleen, thereby reducing the CLL tumour burden.22,23 Improved haemoglobin and thrombocyte levels might be direct results of a reduction in spleen size, with consequent decrease in erythrocyte and thrombocyte degradation by the spleen. Splenic irradiation in CLL might also have more indirect, or abscopal, effects. The term ‘abscopal effect’ was first used by Mole in the 1950s to describe systemic effects after local radiotherapy.24 For example, factors released from irradiated B-CLL cells into their supernatants were shown to inhibit non-irradiated leukaemic cell growth in vitro.25 Furthermore, in the 1980s splenic irradiation was shown to induce shifts in lymphocyte subsets, which was hypothesised to augment anti-tumour responses in lymph nodes and bone marrow, and to have a beneficial effect on normal haematopoiesis, which might be suppressed by autoimmune phenomena.14 Experimental evidence supporting these hypotheses was indirect. From more recent studies it is becoming clear that the interaction between CLL cells and their tissue microenvironment (consisting of amongst others stromal cells, monocytederived nurse-like cells, and T lymphocytes), plays an important role in promoting the survival of CLL cells.26 Irradiation of the spleen could result in disruption of this beneficial microenvironment. To better characterise which mechanisms exactly contribute to the beneficial effects, abscopal or direct, of splenic irradiation, novel studies should be performed.
No significant side effects of splenic irradiation were observed in the four cases presented here. Solely based on our small case series no conclusions can be drawn on the safety of splenic irradiation in CLL. However, also in previous studies side effects were modest, and limited to tiredness, thrombocytopenia, and to a lesser extent neutropenia.12,27 Because of this low toxicity, multiple courses of splenic irradiation can be given. The effectiveness of splenic irradiation in frail CLL patients might be improved in the future by combining splenic irradiation with immunotherapeutic agents targeting the B-cell receptor signalling pathway, which might be better tolerated in frail patients than the combination of immunotherapy with chemotherapy. Alternatively, in the future splenic irradiation might be combined with checkpoint inhibition of PD-1 or PD-L1 (expressed by CLL cells),28 in analogy with the very promising combination of radiotherapy and checkpoint inhibition in the treatment of melanoma.29
In conclusion, although the application of splenic irradiation in CLL is nowadays mostly limited to treat splenomegaly-related symptoms, historic studies and the current results in four elderly CLL patients show that splenic irradiation might also result in prolonged periods of haematological remission and an improved wellbeing with low or no toxicity. We therefore emphasise that this old tool should not be forgotten in the treatment of especially the elderly CLL patient, who frequently presents with multiple comorbidities.
DISCLOSURES
The authors have no competing interests to disclose.
The abstract of this article was presented orally at the 27th ‘Internistendagen’, Maastricht, Netherlands, on 22 April 2015.
REFERENCES