To the Editor,
Dosing of antibiotics can be challenging, as was demonstrated in your journal for vancomycin and intensive care patients by Brinkman et al.1 We would like to warn colleagues for potential underdosing of gentamicin in patients with sepsis, as we recently found in our emergency department.
Aminoglycosides are frequently used in the empirical treatment of sepsis in the emergency department. In our hospital, we aim to prescribe gentamicin 5 mg/kg once daily, to broaden the antibiotic spectrum of amoxicillin/ clavulanic acid.2 Gentamicin is a concentration dependent bactericidal antibiotic. Underdosing will lead to a lower gentamicin peak concentration and consequently to potential treatment failure and increased morbidity and mortality.3,4 Therefore, we investigated actual gentamicin dosing in patients with sepsis in our emergency department.
All patients who received gentamicin at our emergency department (Maastricht University Medical Centre, the Netherlands) from April 2011 to April 2012 were included. We retrospectively retrieved data on body weight, height, gentamicin dose and clinical characteristics from the electronic patient files and electronic prescribing system. To calculate the correct dose of gentamicin (5 mg/kg), actual body weight was used for patients with a body mass index (BMI) < 30 kg/m2 , and adjusted body weight for patients with BMI > 30 kg/m2. 5 Underdosing of gentamicin was defined as at least 10% under the advised dose, i.e. < 4.5 mg/kg.
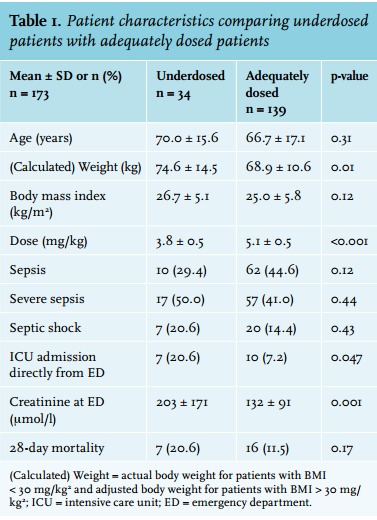
We included 173 patients, of whom 34 (20%) were underdosed. The mean gentamicin dose was 3.8 ± 0.5 mg/kg in the underdosed group, and 5.1 ± 0.5 mg/kg in the adequately dosed group (table 1). There was no difference in severity of sepsis according to the SIRS criteria (i.e. sepsis, severe sepsis, or septic shock) in both groups.6 Mean serum creatinine was higher in underdosed patients (203 ± 171 vs. 132 ± 91 mmol/l, p = 0.001) and underdosed patients were more often directly admitted to the ICU (21% vs. 7% of patients, p = 0.047), which may indicate a worse condition of these patients.
In conclusion, gentamicin is frequently underdosed in patients with sepsis in our emergency department. This leads to lower peak concentrations, which may negatively influence clinical outcome. The higher serum creatinine in gentamicin underdosed patients might suggest that fear of nephrotoxic side effects is an important reason for underdosing. Other reasons might be an incorrect estimation of body weight, which was also seen in patients receiving thrombolysis,7 or rounding down of the gentamicin dose, based on whole ampules (i.e. 80 mg/2 ml).
Given the frequent occurrence of underdosing of gentamicin in our hospital, this could be a concern in other hospitals as well. We suggest that other emergency departments check the doses of aminoglycosides actually given. To improve dosing, standardised weighing before administering gentamicin might be considered. Alternatively, plasma peak concentrations could be useful in the adequate dosing of gentamicin.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES