KEYWORDS
Anti-CD20, anti-IL6, chemotherapy, HIV-1, human herpesvirus 8, multicentric Castleman’s disease
INTRODUCTION
Multicentric Castleman’s disease (MCD) is a lympho - proliferative disorder affecting B-lymphocytes and plasma cells. An infection with the human herpesvirus (HHV)-8, especially in human immunodeficiency virus (HIV)-1 infected patients, has been frequently associated with MCD development.1,2 Three histological categories of MCD are identified: the plasma cell, hyaline vascular and mixed variants. The plasma cell variant is present in 80-90% of MCD cases. An HHV-8 infection results in the production of human and viral (HHV-8 DNA encoded) pro-inflammatory interleukin (IL)6 that induces plasma cell proliferation, and appears to be of importance in MCD pathogenesis.3-5 MCD is diagnosed by histological evidence of affected tissues in patients with pro-inflammatory clinical symptoms.
Despite the ever-increasing number of patients with adequately controlled HIV-1 by combination antiretroviral therapy (cART), MCD incidence in HIV-1 patients is increasing.6 The incidence in HIV-1 patients has been estimated at 2.3 per 10,000 patient-years in the pre-cART era prior to 1996, and 8.3 per 10,000 patient-years since 2000. In the general population, ten-year MCD prevalence is approximately 2.4 per million persons.6,7 The clinical course of MCD is seldom self-limiting and, if left untreated, associated with high mortality rates. However, the optimal treatment for MCD remains unclear.8 MCD treatment strategies include chemotherapy, anti-CD20 antibodies (rituximab) and the use of antibodies directed against IL6 or the IL6 receptor (anti-IL6(R)). This systematic review aims to summarise available evidence of these MCD therapies and their potential complications.
METHODS
The primary purpose of this systematic review was to provide an overview of all conducted trials, prospective and retrospective cohort studies on chemotherapeutic or immunomodulatory (anti-CD20 and anti-IL6(R)) treatments of HHV8-associated and HHV8-unrelated MCD, both in HIV-positive and HIV-negative patients. The study conduct was in accordance with the PRISMA statement for systematic reviews.9
Search strategy
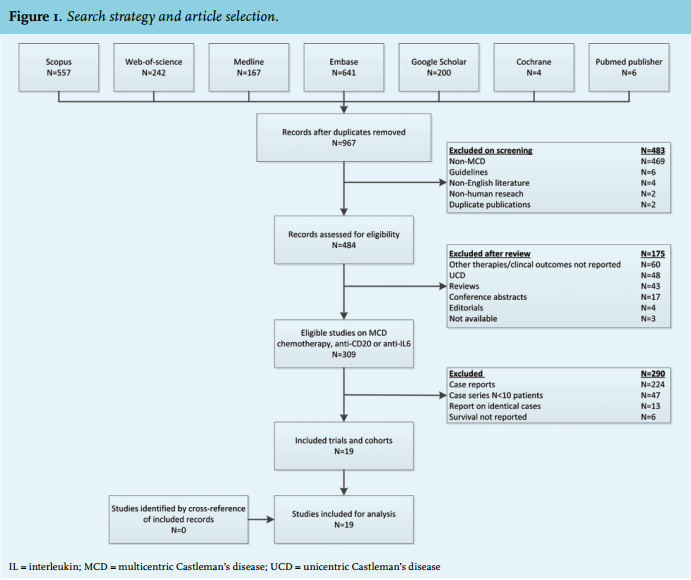
Studies were extracted from an extended search in Embase, Medline (OvidSP), Web-of-Science, Scopus, PubMed publisher, Cochrane Library and Google Scholar up to 16 December 2014. Results were limited to retrospective or prospective cohorts and clinical trials in humans from the English literature. The search was not restricted by age, HIV-1 status, or HHV-8 status. We searched the following medical subject heading terms in titles and abstracts: “Castleman” OR “Angiofollicular lymph node hyperplasia” AND “Chemotherapy” OR “Anti-CD20” OR “Rituximab” OR “Anti-IL6” OR “Tocilizumab” OR “Siltuximab”. Duplicate findings were identified and removed. Initial screening of the titles and abstracts excluded animal studies, guidelines, identical publications and identified studies primarily on MCD. The titles and abstracts of the remaining studies were assessed on eligibility. We excluded studies that did not primarily report outcomes on the clinical effectiveness of chemotherapy, anti-CD20 or anti-IL6(R) for MCD, provided insufficient data on therapy outcomes or were available as conference abstracts only. We assessed the full text of studies on eligibility if the title and abstract were inconclusive. All eligible trials and cohort studies had to report on at least ten MCD patients on identical treatment consisting of chemotherapeutic, anti-CD20 or anti-IL6(R) therapies. Only studies with data on treatment outcomes and survival outcomes were included for the analysis. Case reports were excluded. We identified reports on identical patient series and included the most recent records. The final selected studies for analysis were cross-referenced for potential omitted relevant studies.
Data extraction
The following information was extracted from the studies: principle author, year of publication, study design, number of patients included, patient characteristics (age, gender), HIV-1 infection, HHV-8 status, cART, tissue histology, clinical course, therapy received, and treatment outcomes. The number of deaths and median or mean follow-up time were evaluated in all studies. If available, the reported survival rates were extracted for comparability reasons unless no survival rates were reported and the authors provided an alternative efficacy endpoint. We evaluated incidences of Kaposi sarcoma, lymphoma, and haemophagocytic lymphohistiocytosis (HLH) if reported. The results were reviewed on (pooled) descriptive characteristics and therapy outcomes. The levels of evidence and recommendations were graded according to the Oxford Centre for Evidence-Based Medicine levels of evidence.10 No interferential statistics were computed due to the heterogeneity of study designs and lack of uniform study endpoints.
RESULTS
Study and patient characteristics
Of 1817 studies identified by the search, 309 were eligible studies on MCD chemotherapy, anti-CD20 or anti-IL6(R) (figure 1). These included 224 case reports, 47 case series on less than ten patients, and 13 reports on identical patient series. Nineteen studies, including five trials and 14 cohort studies, were included for analysis and provided data on 666 predominantly male (79.9%) patients with MCD. The level of evidence of all trials was grade 2B because of limited follow-up or absence of control groups. One cohort was grade 2B due to size, reported outcomes, follow-up duration and identification and correction of potential confounders.11 All other cohorts were low-quality studies of grade 4. Median age was 43 (range: 37-65) years. Data on gender and age were not available in one study.12 HIV-1 was excluded by serology in all patients in five studies,13-17 and in 13 of 21 patients in one study.18 One trial did not report HIV-1 status.19 Available HIV-1 test results were positive in 100% of patients in the remaining 11 studies, except in one retrospective cohort study (64% HIV-1 positive).20 In total, 450 patients were HIV-1 positive and 216 were either HIV-1 negative or had an unknown HIV status. Apart from one study,21 all studies were from the cART era and reported cART coverage in these studies was 65.4% (270/430 patients) at MCD diagnosis. The reported HIV-1 RNA suppression rate < 500 copies/ml was 40.8% and median CD4 cell count was 221 (range: 148-398) cells/mm3 . MCD diagnosis was established by histological tissue examination in 98.5% of patients. Results on MCD variants were reported in 64 HIV-1 positive patients,20-23 and 192 HIV-1 negative patients.13,14,16-19 Only the plasma cell and mixed variants were observed in 54.7% and 45.3% of HIV-1 patients respectively. MCD variants in HIV-1 negative patients were 49.5% plasma cell, 25.5% hyaline vascular, and 25.0% mixed variants. Splenectomies were performed in 39 patients and 29/39 were reported in studies conducted prior to 2008. Kaposi sarcoma foci were reported in four studies and apparent in 17 of 91 (18.7%) histologically examined MCD tissues.21,22,24,25 No histopathological evidence for lymphoma was found at MCD diagnosis although 13 studies either did not report results or excluded patients with evidence of lymphoma. The reported HHV-8 detection methods varied. Two studies did not report on HHV-8 status,16,26 two studies omitted the description of the detection methods,19,20 and six studies described multiple HHV-8 detection methods.11,12,15,22-24 Quantitative HHV-8 polymerase chain reaction (PCR) in plasma was used in 11 studies,11,15,17,18,22-25,27-29 including one trial that excluded HHV-8 infected patients.17 ELISA or immunofluorescence antibody assays to latent nuclear antigens were used in three studies,13,22,24 and six studies used HHV-8 PCR or immunohistochemistry on biopsy tissues.11,12,15,21,23,24 Excluding the studies that did not report or include HHV-8 patients,16,17,26 HHV-8 test results were available for 416/525 patients (79.2%) and HHV-8 was demonstrated in 83.4% (347/416) of patients. These patients included 99.7% (326/327) of HIV-1 positive patients compared with 24.4% of HIV-1 negative patients with HHV-8.
MCD therapy and outcome
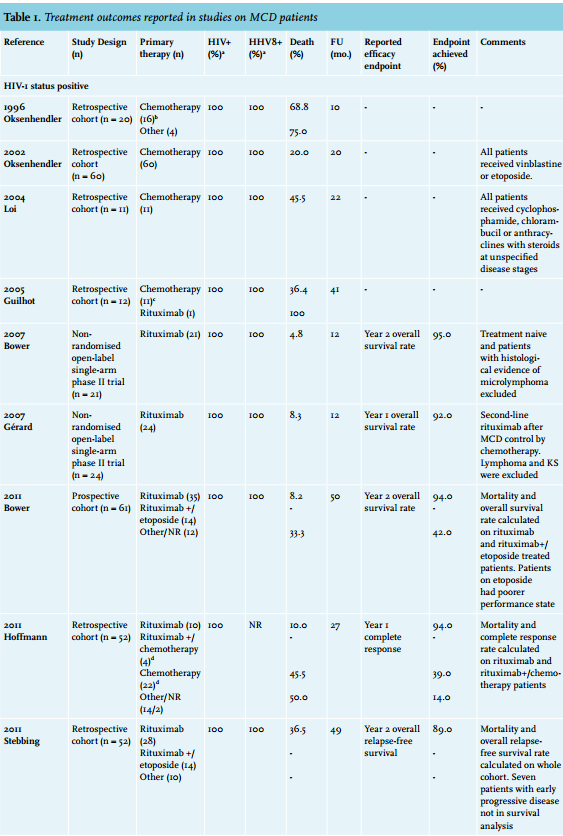
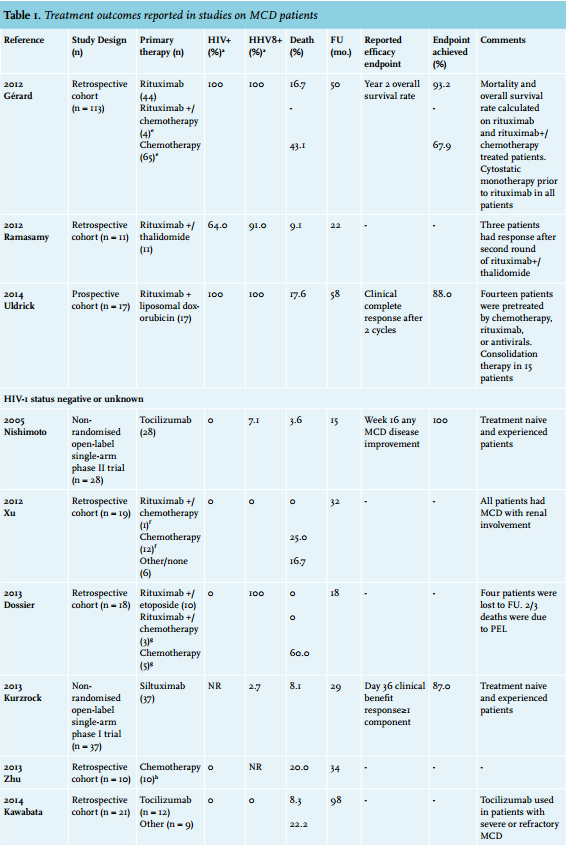
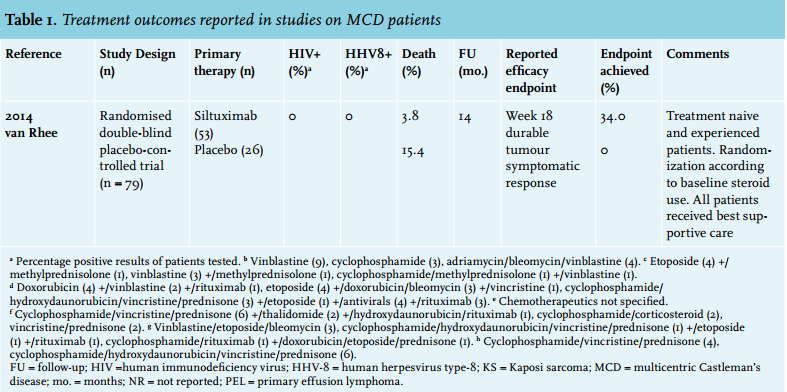
MCD treatments, survival and main therapy outcomes are shown in table 1. Results are categorised according to HIV-1 status. Six cohort studies were predominantly on chemotherapy alone,12,14,16,21,22,29 nine studies were either on rituximab alone,23,24 or on rituximab/chemotherapy combined,11,15,20,25-28 and four studies, including the only randomised placebo-controlled double-blind clinical trial on MCD therapy, were on anti-IL6(R).13,17-19 The cumulative number of patients treated by chemotherapy was 212, by rituximab this was 241 (including 163 patients on rituximab alone), and 130 were treated by anti-IL6(R). Eighty-three patients were treated by other or unreported therapies or received palliative care only. Of 212 patients on chemotherapy, 107 were treated by single cytostatics to control MCD recurrences including vinblastine, cyclophosphamide, chlorambucil, etoposide, doxorubicin and vincristine. Combination chemotherapy was used in 40 patients as first- or second-line regimens. One study did not specify the chemotherapies used in 65 patients.11 Excluding prior corticosteroid exposure, rituximab was used as first-line therapy in 151 patients as single agent (n = 95) or in combination with chemotherapy (n = 56), predominantly etoposide (n = 36). As second-line therapy, rituximab monotherapy was used in 68 patients and rituximab/chemotherapy (predominantly liposomal doxorubicin) combined in 22 patients with (chemo)therapy dependent MCD. The majority of patients (105/130, 80.8%) on anti-IL6(R) therapy received prior systemic therapies. The overall all-cause mortality rate was 137/666 patients (20.6%) at a median follow-up of 27 months. Mortality rates were 25.3% in HIV/HHV-8 positive and 10.6% in HIV-1 (and for the large majority HHV-8) negative patients. The causes of death were progressive MCD in 17.5% and 34.8% of HIV-1 positive patients and HIV-1 negative patients, respectively, infections (or AIDS in HIV-1 positive patients) in 12.3% and 13.0%, multi-organ failure in 4.4% and 4.5%, progression to lymphoma in 39.5% and 8.7%, and unreported or unknown in 21.9% and 39.0%. Kaposi sarcoma was the cause of death in 5/114 (4.4%) HIV-1/HHV-8 positive patients only. The mortality rates according to treatment modalities received during reported follow-up were 36.8% for chemotherapy alone, 10.1% for rituximab with or without chemotherapy, 7.7% for anti-IL6(R) and 30.1% for other therapies. Of note, one cohort study did not specify deaths according to therapy modalities and could not be used.28
Furthermore, another cohort study only reported on deaths of MCD patients that developed non-Hodgkin’s lymphoma.12 Ten studies defined endpoints that showed broad variety in definitions. Overall, first- or second-line rituximab containing therapy was more able to sustain remission and increase survival than chemotherapy alone, at least in HHV-8 positive, and often HIV-1 positive, MCD patients. The reported proportions of patients who achieved the endpoints were at least 88.0% when rituximab was part of the treatment, and at the most 67.9% with chemotherapy alone. For anti-IL6(R) monotherapy, the majority of patients achieved improvement on at least one disease component although durable tumour and symptomatic responses remained around 40% in this highly pre-treated group of predominantly HIV-1 and HHV-8 negative MCD patients.
Kaposi sarcoma, HLH and lymphoma
Kaposi sarcoma, HLH and lymphoma were frequently diagnosed prior to MCD diagnosis or during follow-up. Excluding the three antiIL6(R) trials and four studies that did not report on Kaposi sarcoma,14,16,18,28 Kaposi sarcoma was apparent in 244 of 429 patients. Progression of Kaposi sarcoma during follow-up occurred in 55 (12.8%), predominantly HIV-1 positive (96.4%), MCD patients. The majority of Kaposi progressions (67.3%) were observed in studies of patients treated with rituximab. In the studies that specifically reported on lymphoma development during MCD follow-up (n = 416), the incidence was 15.1%. Three studies reported on HLH, which was diagnosed in 34.3% of 143 patients at MCD diagnosis or during follow-up.11,15,22
DISCUSSION
The current systematic review indicates that the use of rituximab appears to provide a survival benefit, both in HIV-1 positive and HIV-1 negative, HHV-8 associated MCD patients in first- or second-line therapy (Grade B recommendation). Anti-IL6(R) showed promising results in controlling disease activity, at least in HIV-1 and HHV-8 negative patients (Grade B recommendation). The optimal treatment of HHV-8 positive and HHV-8 negative MCD patients remains unclear and largely based on low-quality evidence. Etoposide and liposomal doxorubicin have been used with favourable results in combination with rituximab in HHV-8 associated MCD (Grade C recommendation). The use of chemotherapy alone was generally associated with higher mortality rates than in combinations with rituximab. This indicates that it might be preferable not to use chemotherapy without rituximab (Grade C recommendation). Despite treatment, the clinical course of MCD is frequently complicated by exacerbations of Kaposi sarcomas, lymphoma development, or HLH, and the mortality remains high.
Disease progression to (often HHV-8 related) lymphoma is frequently observed in MCD and appears to be partially prevented by including rituximab in MCD treatment. In MCD, HHV-8 infected B-lymphocytes are able to coalesce and form microscopic lymphoma, which may express the CD20 antigen.5,30,31 Ongoing IL6 receptor activation might be involved in the lymphoproliferative differentiation of these B-cells. Rituximab’s protective effect could be due to the resulting HHV-8 infected B-lymphocyte depletion, which decreases cytokine levels involved in further B-cell proliferation. Despite the effect of rituximab on lymphoma development, HLH and Kaposi sarcoma are prevalent concomitant clinical complications in MCD. Kaposi sarcoma seems to be related to the rituximab exposure, and almost exclusively in HIV-1 infected patients. HIV-1 and HHV-8 can both trigger HLH, which is associated with a high mortality rate.32 The combination HHV-8 infection and IL6 overproduction in MCD could result in a dysfunctional cascade of cytokine overproduction with T-lymphocyte and macrophage activation causing HLH, especially in immunocompromised HIV-1 patients.33-36 Furthermore, a possible relation has been observed between low B-lymphocyte counts and increased risk for Kaposi sarcoma development with increased expression of HHV-8 gene products in Kaposi sarcomas after rituximab therapy.37-39 A marked decrease in Kaposi sarcoma flares was observed if rituximab was combined with single-agent chemotherapies, mainly etoposide. The clinical implications of these observations are unclear. In our opinion, HHV-8 positive MCD patients should be evaluated for clinical signs of Kaposi sarcoma or its presence in tissue biopsy prior to the initiation of rituximab. If Kaposi sarcomas are present, the concomitant administration of chemotherapeutics (etoposide, liposomal doxorubicin or paclitaxel) might be recommended. However, the possible benefit of adding chemotherapeutics to rituximab on Kaposi flares or survival needs to be further evaluated. Furthermore, the effects of HHV-8 suppression by antiviral agents on Kaposi sarcoma and HLH development in the context of rituximab therapy for MCD is yet unknown. Last, the usefulness of cytokine levels and HHV-8 viral load for the monitoring of treatment effect, disease activity or for predicting patients at risk for MCD relapse after clinical remission and development of subsequent lymphoma, Kaposi sarcoma or HLH warrants further evaluation.40,41
The monoclonal antibodies against IL6 and the IL6 receptor, siltuximab and tocilizumab, are not yet approved for the European market for the treatment of MCD. Siltuximab has a favourable opinion based on the benefit-to-risk balance and European market approval is recommended.42 Tocilizumab has only been approved for the treatment of rheumatoid arthritis. Evidence is available from trials on the subgroup of MCD patients without HIV-1 or HHV-8 and the efficacy of these drugs in other patient groups remains to be elucidated. Issues on drug safety especially for the orphan medicine siltuximab are another important issue because of the limited experience with this drug. Additional trials on tocilizumab and siltuximab in MCD are ongoing.43,44
The overall level of evidence of the studies was low and no definite conclusions can be drawn on the available evidence. All studies were obviously biased in several ways. Important confounders as HHV-8 status, HIV-1 infections, Karnofsky performance scores, detailed treatment information and the presence of Kaposi sarcoma or microlymphomas in tissue examinations were not uniformly investigated or reported. Unmeasured confounders have likely occurred during the covered time period, which make comparisons difficult. The large number of case reports and case series indicate publication bias, which cannot be evaluated due to the absence of registration databases for these studies. Selection bias of patients is a major limitation for interpreting the studies. The results of the cohort studies are predominantly influenced by possible treatment-allocation bias; the patients at highest risk for death received palliative care only or had aggressive and often fatal lymphomas for which chemotherapy was warranted. Therefore, the results should be interpreted cautiously. Lastly, an in-depth evaluation of treatment responses according to HHV-8 status might have been the preferred method from a pathophysiological point of view. The large amount of missing data regarding HHV-8 status, the heterogeneous use of variable HHV-8 detection methods, and other study limitations hindered this separation.
CONCLUSION
Based on the results of the present systematic review we cannot provide conclusive evidence-based treatment recommendations for optimal MCD therapy in HIV-1 infected or uninfected patients. Although the available evidence is of low quality, the use of rituximab appears to provide a survival benefit in HHV-8 associated MCD, and anti-IL6(R) therapy might offer a treatment option after first-line treatment failure for HIV-1 negative patients without HHV-8 associated MCD.
ACKNOWLEDGEMENTS
We thank Wichor Bramer from the Erasmus University Medical Centre for his expertise in biomedical information and systematic literature search.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES
APPENDIX
Search terms used in the medical databases for the literature search in the systematic review on the treatment of multicentric Castleman’s disease.
Embase.com
(‘angiofollicular lymph node hyperplasia’/de OR (((angiofollicul* OR angiolymphoid* OR angiomat* OR ‘Giant Lymph’) NEAR/3 (hyperplas* OR hamarto*)) OR Castleman* OR Castelman*):ab,ti) AND (chemotherapy/ exp OR rituximab/de OR siltuximab/de OR tocilizumab/de OR ‘monoclonal antibody’/de OR ‘CD20 antibody’/de OR (chemotherap* OR rituximab OR ((‘cd 20’ OR cd20 OR ‘il 6’ OR ‘interleukin 6’ OR il6) NEAR/3 (anti*)) OR siltuximab OR tocilizumab OR (monoclonal NEAR/3 antibod*)):ab,ti) AND (‘clinical study’/exp OR ‘cohort analysis’/de OR ‘follow up’/ de OR (clinical* OR cohort* OR longitudinal* OR (follow* NEXT/1 up) OR followup* OR prospective* OR retrospective* OR random* OR rct* OR placebo* OR ((double* OR single* OR triple*) NEAR/3 blind*) OR (controlled NEAR/3 stud*) OR trial*):ab,ti) AND [english]/lim
Medline (OvidSP)
(“Giant Lymph Node Hyperplasia”/ OR (((angiofollicul* OR angiolymphoid* OR angiomat* OR “Giant Lymph”) ADJ3 (hyperplas* OR hamarto*)) OR Castleman* OR Castelman*). ab,ti.) AND (Chemotherapy, Adjuvant/ OR “Antineoplastic Combined Chemotherapy Protocols”/ OR exp “Antibodies, Monoclonal”/ OR (chemotherap* OR rituximab OR ((“cd 20” OR cd20 OR “il 6” OR “interleukin 6” OR il6) ADJ3 (anti*)) OR siltuximab OR tocilizumab OR (monoclonal ADJ3 antibod*)).ab,ti.) AND (exp “Clinical Trial”/ OR exp “Cohort Studies”/ OR (clinical* OR cohort OR longitudinal* OR (follow* ADJ up*) OR followup* OR prospective* OR retrospective* OR random* OR rct* OR placebo* OR ((double* OR single* OR triple*) ADJ3 blind*) OR (controlled ADJ3 stud*) OR trial*).ab,ti.) AND english.la.
Cochrane
((((angiofollicul* OR angiolymphoid* OR angiomat* OR ‘Giant Lymph’) NEAR/3 (hyperplas* OR hamarto*)) OR Castleman* OR Castelman*):ab,ti) AND ((chemotherap* OR rituximab OR ((‘cd 20’ OR cd20 OR ‘il 6’ OR ‘interleukin 6’ OR il6) NEAR/3 (anti*)) OR siltuximab OR tocilizumab OR (monoclonal NEAR/3 antibod*)):ab,ti)
Web-of-science
TS=(((((angiofollicul* OR angiolymphoid* OR angiomat* OR “Giant Lymph”) NEAR/3 (hyperplas* OR hamarto*)) OR Castleman* OR Castelman*)) AND ((chemotherap* OR rituximab OR ((“cd 20” OR cd20 OR “il 6” OR “interleukin 6” OR il6) NEAR/3 (anti*)) OR siltuximab OR tocilizumab OR (monoclonal NEAR/3 antibod*))) AND (clinical* OR cohort OR longitudinal* OR “follow up” OR followup* OR prospective* OR retrospective* OR random* OR rct* OR placebo* OR ((double* OR single* OR triple*) NEAR/3 blind*) OR (controlled NEAR/3 stud*) OR trial*)) AND LA=english
Scopus
TITLE-ABS-KEY(((((angiofollicul* OR angiolymphoid* OR angiomat* OR “Giant Lymph”) W/3 (hyperplas* OR hamarto*)) OR Castleman* OR Castelman*)) AND ((chemotherap* OR rituximab OR ((“cd 20” OR cd20 OR “il 6” OR “interleukin 6” OR il6) W/3 (anti*)) OR siltuximab OR tocilizumab OR (monoclonal W/3 antibod*))) AND (clinical* OR cohort OR longitudinal* OR “follow up” OR followup* OR prospective* OR retrospective* OR random* OR rct* OR placebo* OR ((double* OR single* OR triple*) W/3 blind*) OR (controlled W/3 stud*) OR trial*)) AND LANGUAGE(english)
PubMed publisher
((((angiofollicul*[tiab] OR angiolymphoid*[tiab] OR angiomat*[tiab] OR Giant Lymph*[tiab]) AND (hyperplas*[tiab] OR hamarto*[tiab])) OR Castleman*[tiab] OR Castelman*[tiab])) AND ((chemotherap*[tiab] OR rituximab[tiab] OR ((cd 20*[tiab] OR cd20[tiab] OR il 6*[tiab] OR interleukin 6*[tiab] OR il6[tiab]) AND (anti*[tiab])) OR siltuximab[tiab] OR tocilizumab[tiab] OR monoclonal antibod*[tiab])) AND ((clinical*[tiab] OR cohort[tiab] OR longitudinal*[tiab] OR follow up*[tiab] OR followup*[tiab] OR prospective*[tiab] OR retrospective*[tiab] OR random*[tiab] OR rct*[tiab] OR placebo*[tiab] OR double blind*[tiab] OR single blind*[tiab] OR triple blind*[tiab] OR controlled stud*[tiab] OR trial*[tiab])) AND english[la] AND publisher[sb]
Google scholar
Castleman chemotherapy|rituximab|siltuximab|toci lizumab|”monoclonal|CD20 antibody|antibodies”|”anti il-6|interleukin-6|il6” clinical|cohort|”follow up”|prospecti ve|retrospective|randomized|randomised|random|rct