KEYWORDS
Critical care, highly resistant microorganisms, HRMO, length of stay, surveillance, isolation
INTRODUCTION
Antibiotic resistance in the critical care population is an ever-increasing problem.1 The high use of antimicrobial therapy in the intensive care unit (ICU),2 the large number of invasive procedures, the density of a susceptible patient population, the severity of underlying illness, and flaws in infection control measures are all contributing factors resulting in ICUs as ‘epicentres’ of antimicrobial resistance in hospitals.3,4 ICUs are considered generators of antimicrobial resistance.3 In addition to acquisition of HRMOs in the ICU, part of the resistance problem is imported to the ICU through already colonised or infected patients admitted from other hospitals, general wards, or from the community.5
This continuous and rising threat of antimicrobial resistance is of relevance considering the outcome in patients infected with resistant rather than susceptible microorganisms is worse.6 Measures to prevent cross-contamination include surveillance, barrier precautions and antibiotic stewardship. All preventive measures are labour intensive, costly and some are patient unfriendly. Resistance to first-line antibiotics urges the use of ‘rescue’ or second-line antibiotics with little hope of new effective alternatives in the near future.7
The incidence and characteristics of resistance can vary widely depending on local circumstances. According to European surveillance data, the Netherlands, along with Scandinavian countries, is considered an area with low incidence of antimicrobial resistance for Gram-positive as well as Gram-negative bacteria.8 However, even in the Netherlands, prevalence of antimicrobial resistance in the community is not negligible, and is emerging.9-11
We evaluated the incidence of HRMOs in our ICU to quantify the total burden of HRMOs, to clarify the local distribution of different categories of HRMOs and the proportion of imported versus acquired HRMOs in our ICU. Furthermore, we evaluated the outcome of patients affected by colonisation or infection with any HRMO vs. controls in terms of ICU mortality and length of stay (LOS) in the ICU. Finally, we wanted to characterise this subpopulation colonised or infected with an HRMO to enable better a priori recognition of affected patients, thus rendering better opportunities for adequate treatment and infection control.
MATERIALS AND METHODS
This is a single-centre study involving prospective data collection from 1 October 2009 to 31 January 2010 in an academic teaching hospital with 40 critical care beds distributed over 4 units (medical, cardiothoracic, neurological, and general surgery). All four units consist of a large multi-bed floor combined with a few rooms for isolation. On the floors, standard hygienic procedures are maintained. Annually, between 2500 and 3000 patients are admitted. All patients admitted in the four-month study period were included for analysis. The study was approved by the ethics committee and the requirement of informed consent was waived. We recorded baseline characteristics including sex, age, referring speciality, unit of admission, APACHE II score, date and source of admission (emergency department or general ward vs. other hospital). APACHE II score was not recorded for cardiosurgical patients because this score is not validated for this subgroup. Of note, patients from various sources were admitted to the four separate units, e.g. the cardiothoracic unit did not only admit cardiothoracic surgery patients but other patients as well. Patients were considered referred from another hospital if they were transferred either directly to the ICU or indirectly through another ward in our hospital. The vast majority of this last group were admitted to the general ward for less than a week before admission to our ICU.
All cultures taken either by indication or in the context of our structured surveillance program were evaluated. Surveillance screening included cultures from throat, nose, rectum, sputum and urine on admission, followed by cultures from throat, nose, rectum and sputum on day four and twice weekly thereafter during the stay in the ICU. Surveillance cultures were obtained from those patients with an anticipated stay of 48 hours or more on the day of admission. Patients referred from elsewhere were included in surveillance screening on the day of admission regardless of anticipated or actual length of stay. Culture results were retrieved from the database of the department of medical microbiology. Susceptibility testing was done according to European guidelines (European Committee on Antimicrobial Susceptibility Testing, EUCAST).
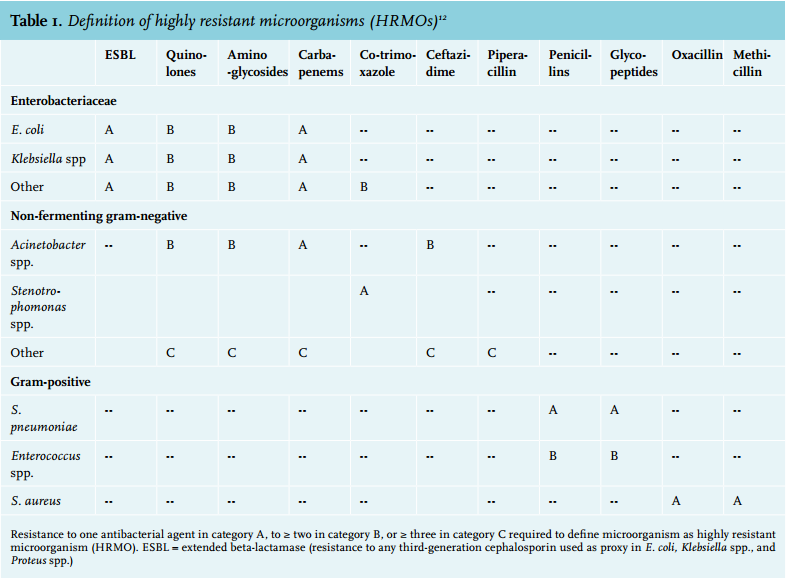
HRMOs were defined by criteria issued by the Dutch Working Party on Infection Prevention (table 1).12 All patients colonised or infected with an HRMO were placed in full contact isolation, as dictated by our protocol for infection prevention. A patient could be included only once in the study group; subsequent readmissions of the same patient were excluded from the study group but were analysed nevertheless. Only the first positive culture for any HRMO in an individual was recorded; subsequent cultures with the same organism were regarded as the same event. Different species of HRMOs within one patient were recorded as separate events. No distinction was made between either colonisation or infection with an HRMO. Of the patients with an HRMO, further details such as antibiotic use during the hospital stay and medical history were retrieved from the patient’s file. Other outcome measures for the entire study population included ICU mortality and LOS on the ICU.
We tried to identify clusters of HRMOs by analysing whether identical species of HRMOs were cultured in different patients during their ICU stay on the same unit. Statistical methods included the χ2 -test, Fisher’s exact test, Student’s t-test, Mann-Whitney U-test and Wilcoxon rank test, where appropriate, using Minitab® Release 14.1 and Graph Pad Prism (Prism 5 for Windows, version 5.04, Nov 6 2010) software.
RESULTS
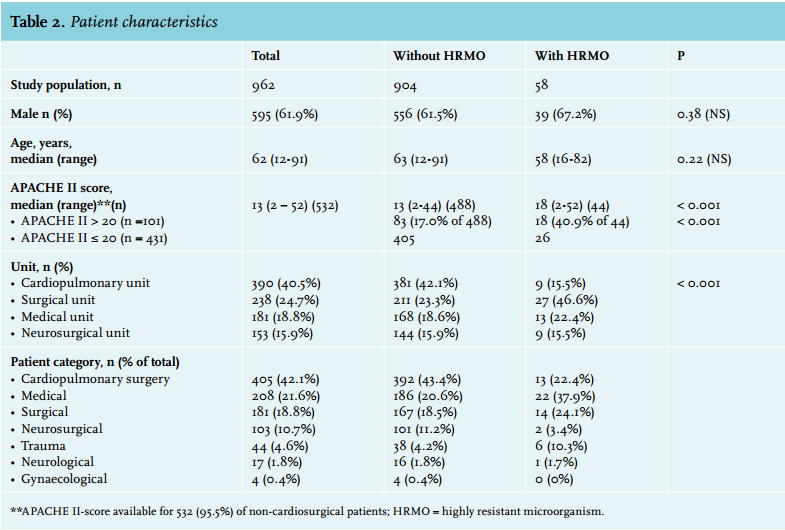
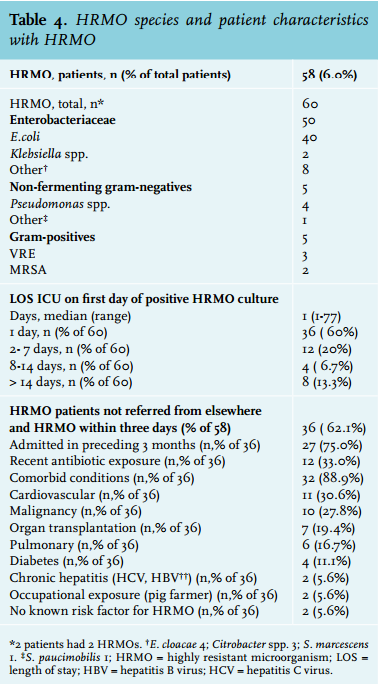
A total of 1061 admissions were recorded, 91 of which were re-admissions within the study period; hence 962 admitted patients were included in the study population (table 2). Baseline characteristics are presented in table 2 and 3. In 58 (6.0%) patients an HRMO was found (in total 60 HRMOs; two patients had two different HRMOs). For distribution of HRMO species we refer to table 4. The distribution of these 58 patients according to unit and patient category is depicted in table 2.
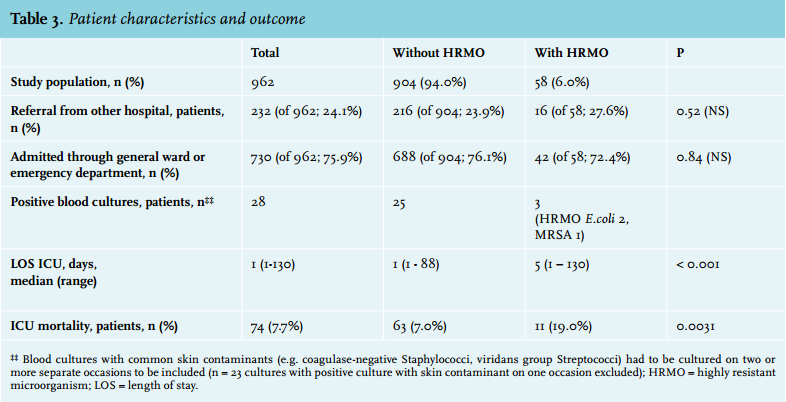
Of 232 patients (24.1%) referred from another hospital, 16 patients were colonised with an HRMO during their stay in our ICU (6.9%), compared with 42 out of 730 patients (5.8%) referred from our hospital (p = 0.52). In those patients with any HRMO (n = 58), 47 patients (82.8%) were found to have an HRMO within the first three days of ICU stay. Of these, 11 (23.4%) were referred from another hospital: 36 (76.6%) were admitted from a general ward of this hospital or from the emergency department.
Of those not referred from elsewhere and found positive for an HRMO within three days (n = 36), 32 patients (88.9%) had one or more comorbid conditions (table 4). In this group of 36 patients, 27 patients (75.0%) had been admitted in the three months preceding current admission to the ICU; 12 patients (33.3%) had received antibiotics in the months preceding ICU admission. Two patients (of 36, 5.6%) were farmers working with livestock (pigs); both were found to be methicillin-resistant Staphylococcus aureus (MRSA) positive. Two (of 36, 5.6%) had no comorbid conditions, no recent hospital admission, no recent antibiotic treatment and no occupational exposure to HRMOs.
Median LOS for all ICU patients was 1 day (range 1-130 days, mean 4 days). LOS in the ICU for HRMO-positive patients was significantly longer (median 5 days, range 1-130, mean 16 days) compared with HRMO-negative patients (median 1 day, range 1-88, mean 3 days) (p = 0.000) (table 3).
LOS in the ICU at the time of first positive culture for any HRMO was 1 day in 36 (60%), 2-7 days in 12 (20%), 8-14 days in 4 (7%) and more than 14 days in 8 (13%) (table 4). Patient categories with most HRMO-positive patients were medical (22 out of 208, 10.6%), surgical (14 out of 181, 7.7%) and trauma (6 out of 42, 13.6%). Units with most HRMO-positive patients were the surgical unit (27 out of 218, 11.3%) and the medical unit (13 out of 181, 7.2%).
Of patients admitted to our ICU for more than 14 days, 18 of 57 (31.6%) were found to have any HRMO during ICU stay vs. 31 of 840 (3.7%) patients staying 7 days or less in our ICU ( p < 0.0001).
APACHE II score for HRMO-positive patients (available in 57 patients) was significantly higher (median 17, mean 19, range 2-52) compared with the APACHE II score for HRMO-negative patients (available in 875 patients) (median 13, mean 13, range, 2-44) (p = 0.000). Overall ICU mortality was 74 (7.7%); mortality was significantly higher in patients with HRMO (11 out of 58, 19.0%) than patients without HRMO (63 out of 904, 7.0%) (p = 0.0031) (table 3).
Further, 25 patients had a positive blood culture with a susceptible microorganism and three other patients had a positive blood culture with an HRMO (E. coli 2, MRSA 1). In the readmitted (excluded) patient group (n = 99), 16 patients (16.2%) had any HRMO (E. coli 6, Klebsiella spp. 3, other Enterobacteriacea 3, Pseudomonas spp. 1, other non-fermenting Gram-negatives 1, vancomycin-resistant Enterococci 3). This percentage of HRMO-positive patients is significantly higher compared with the percentage of HRMO-positive patients in the study group (6.0%, p = 0.0002) In this study, we could not identify patient characteristics with sufficient specificity and sensitivity to predict HRMO carriage. During the study period, we did not find clusters of identical HRMOs indicating an outbreak.
DISCUSSION
In this single-centre prospective study on the burden of HRMOs in critical care patients in an area where HRMOs are non-endemic,8,13 it is an important finding that more than half of HRMO-positive patients were identified from cultures taken on admission. This finding suggests that an important part of antibacterial resistance is imported to the ICU, rather than acquired during the ICU stay. Indeed, hospitalisation on a general ward prior to ICU admission is a recognised risk factor for HRMO acquisition14 and although the proportion of HRMOs introduced onto the ICU through already colonised or infected patients has been quantified in studies for MRSA,15 its contribution for all HRMOs has, to the best of our knowledge, not been clearly elucidated as yet in our region. Of all patients admitted through the emergency department or general ward, 36 (out of total 932, 3.7%) had an HRMO within three days of ICU stay. Two (of 36, 5.6%) of these patients had no comorbid conditions, no recent hospital admission, no recent antibiotic treatment and no occupational exposure to HRMOs. Although a minority, this underscores the fact that HRMO is not restricted to the hospital, even in our area of low antibiotic resistance. Indeed, prevalence of antimicrobial resistance in the community, for instance carriage of extendedspectrum beta-lactamases-producing Enterobacteriaceae, is considerable, where contribution of contaminated foods – mainly poultry – and travel, remains to be elucidated.9-11
Only three patients had a proven infection (bacteraemia) with any HRMO, therefore colonisation appears to be far more frequent than a serious infection. That HRMO-positive patients have a higher mortality might in part be explained by the fact that sicker patients are more often colonised with any HRMO. Indeed, in our study population those with an HRMO had a significantly higher APACHE-II score than those without HRMO (table 2). In our cohort, Gram-negative bacteria comprised the largest part of all HRMOs. This is in line with the trend towards more Gram-negative antibiotic resistance in European ICUs, with a stabilisation or decrease in Gram-positive antibiotic resistance.1,16 Recently, others described cephalosporin and aminoglycoside resistance in a substantial number of critically ill patients colonised with Enterobacteriaceae (15 and 10%, respectively) on ICU admission in a large Dutch multi-centre trial.17
We could not identify clusters of HRMO. Therefore, the hygiene measures set forth to contain the spread of HRMOs appeared sufficient in this study period. Our finding that a substantial part of HRMOs are imported into the ICU underscores the imperative need to ensure strict application of hygienic practices, such as hand washing, as well as excellent use of antibiotic stewardship throughout medical care, inside and outside the hospital. Furthermore, this finding highlights the importance of a conscientious surveillance program on the ICU. Along this line, surveillance screening before possible ICU admission in specific populations on medical and surgical wards, or in patients with a high risk of community-acquired HRMO, could be worthwhile in order to prevent cross-contamination on these wards and on the ICU. Indeed, in the Netherlands, a surveillance program comparable to our practice on the ICU is carried out on haemato-oncology and dialysis wards as well. Likewise, it is common practice to screen those with occupational exposure to livestock known to have a high carriage rate of MRSA prior to or at hospital admission.18 Expanding surveillance to other high-risk populations, for instance those admitted to a surgical ward for an extended period, especially when receiving antibiotics, might be beneficial. Some variables have been recognised as risk factors for carriage of HRMOs upon ICU admission, such as prior antimicrobial treatment, prior hospitalisation, and residence in a nursing home.5 However, due to sample size, we could not extract patient characteristics from our study population to predict HRMO carriage. It might be helpful to further characterise those patients at risk for HRMO carriage in the context of a larger epidemiological study. This could lead to more differentiated isolation procedures and a more sophisticated choice of antibiotics in case of a proven or suspected infection. Further studies, however, do necessitate a uniform definition of ‘highly resistant’ enabling meaningful comparisons and data aggregation; currently, a wealth of definitions are being applied in the literature.19
There are some limitations to our study, the most important being that it is a single-centre study with a relatively small sample size. It is important to note that patients with an intended stay of two days or less are not included in the surveillance program, unless transferred from another hospital; positive cultures could thus have been missed in these patients. In this group of patients with a short LOS in the ICU, these potential false-negatives would contribute to our finding that a substantial number of HRMO-positive patients are found to be as such in the first days of admission. As our surveillance program is robustly implemented in our daily practice, it is unlikely that patients were missed out of this program for procedural reasons. Some patients underwent surveillance screening despite a short stay of 48 hours or less on the ICU. We did not differentiate between colonisation and infection with any HRMO. Causality between occurrence of an infection with an HRMO and worse outcome in the HRMO group can thus not be proven in this observational study. We did not analyse all known risk factors for HRMO carriage (referral from a nursing home was not recorded); due to sample size, subgroup analyses were not feasible. It could be of benefit to further characterise those at risk of harbouring infection or colonisation with an HRMO, using a uniform international definition of HRMO, with expanding surveillance in high-risk groups outside the ICU, in order to enable maximum precautionary measures and give optimal antibiotic treatment. This combination of surveillance and timely isolation can prevent further spread of HRMOs, our biggest challenge in infection control in critically ill patients in the years ahead.
CONCLUSION
This observational study suggests that HRMOs on the ICU are quite often imported and not only acquired during the stay in the ICU. Gram-negative HRMOs were more abundant than Gram-positive and are of clinical significance even in a non-endemic area. Although most patients with any HRMO had comorbid conditions, were recently admitted to a hospital, had received antibiotics prior to ICU admission, or had occupational exposure to an HRMO, a small minority had no relevant history. Our findings underscore the importance of infection control and optimal surveillance on admission to the ICU.
ACKNOWLEDGEMENTS
We would like to thank Mr. M. Lazonder for building the database and Mr. H. van Assen for providing APACHE II scores of included patients. Furthermore, we wish to thank Ms. K. Glatman for correcting the English text.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES