KEYWORDS
Antibiotic prescription, drug utilisation, antibiotic stewardship, point prevalence survey, Netherlands
INTRODUCTION
The causal relation between the development of antibiotic resistance and the use of antibiotics is well accepted and multifactorial. In the hospital setting as well as the outpatient setting, unnecessary or inappropriate antibiotic prescribing is common.1-3
To curb the development of antibiotic resistance and reduce the unnecessary use of antibiotics, the Dutch Working Party on Antibiotic Policy (SWAB) recently developed a viewpoint document, which describes the antimicrobial stewardship policy needed for Dutch hospitals. To establish an efficient antimicrobial stewardship program in the hospital, the first step is to identify current institutional resistance patterns and antibiotic usage rates. In addition, it is important to identify targets for quality improvement. Not every hospital requires the same level of intervention and, therefore, an institutional stewardship program should be tailored for each hospital to their own problem pathogens and local overuse of particular classes of drugs in specific patient groups or treatment indications.4
In order to obtain a clear overview of hospital antibiotic prescribing at the patient level, the European Centre for Disease Prevention and Control (ECDC) has developed a standardised data collection technique at the patient level to measure total antibiotic consumption, including indications and method of use. The aim of a point-prevalence survey (PPS), according to the ECDC, is to provide a relatively fast and cheap way to evaluate total antibiotic use, and indications for prescription.5
Publications of a single-centre PPS presenting results of antibiotic consumption are scarce, especially in a setting with low antibiotic consumption and low antibacterial resistance rate. The objectives of this study were to obtain an inventory of antibiotic use in a university hospital and to identify targets for quality improvement of prescription by using a PPS.
METHODS
Design and setting
A point-prevalence study was performed at the Radboud University Medical Centre Nijmegen (Radboudumc, 953 beds). This is one of the largest hospitals in the Netherlands, providing supra-regional tertiary care for a population ~2.5 million residents of the south-eastern part of the country. Antimicrobial guidelines for the most common infectious diseases were introduced in the hospital more than 30 years ago, and have been revised at regular intervals. Antimicrobial guidelines in the Radboudumc are, except for small revisions regarding local restrictions, based on the guidelines developed by the SWAB (http:// www.swab.nl). At present, the electronic version of the antimicrobial guidelines in the hospital is easily accessible on the internet, and available on every computer in the Radboudumc. At the time of this study, the overall antibiotic consumption for the Radboudumc was 65.2 defined daily dose/100 bed-days. For this study, no approval of the local medical ethics committee (CMO Arnhem-Nijmegen) was required, since it was part of quality control of drug utilisation, observational in nature, data used for this study were already available in the electronic patient records, and data were processed anonymously. Department heads were notified by a letter, explaining the aim of the study.
Data collection
A PPS, using the ECDC patient-based audit tool for antibiotic consumption as guideline, was completed on 15 May 2013. For all patients who were on antibiotics at the time of the survey and admitted to the hospital for > 24 hours, data were collected through screening of medical records by a multidisciplinary team, comprising infectious disease specialists (IDS: medical microbiologists/infectious disease physician) and hospital pharmacists. Whenever the reason for treatment was not documented, the attending physicians were contacted in order to obtain missing information. To be included in the study, patients had to be admitted to the hospital for at least 24 hours and still be present at 08.00 a.m. on the day of the study. If patients were temporarily away from the wards for diagnostics and procedures, or at home for a few hours, they were still included. Outpatients, patients in day care (e.g. haemodialysis), and patients in psychiatric wards were excluded. Antibiotics belonging to group J01 (antibacterials for systemic use) of the Anatomic Therapeutic Chemical (ATC) classification system from the World Health Organisation (WHO) Collaborating Centre for Drug Statistics Methodology were included in the study.6 Rifamycin (J04AB03) was included if used for infections other than those caused by mycobacteria. When multiple antibiotics had been prescribed to a patient, all antibiotics were recorded. Antifungal or antiviral therapies, as well as antibiotics used for non-systemic selective digestive tract decontamination, and antibiotics used as prokinetics were excluded.
Optimal antibiotic use and standards for prophylaxis were based on the hospital guidelines. Guideline compliance can be defined as prescribing the correct antibiotic, according to the hospital guidelines, and assessment was done based only on the information written in the patient records. Guideline compliance was classified into four categories: (I) according to hospital guidelines, (II) recommended by an IDS, (III) according to ward-specific policies, (IV) other (i.e. recommendation of supervisor; international consensus). Categories I, II, and III were considered to be compliant with the guidelines, while category IV was considered non-compliant, unless deviations were based on valid grounds and no other recommendation was available. A more detailed description on data collection can be found in the supplementary data.
Data analysis and statistics
Data were entered into a database, double checked by the investigator, and analysed using IBM SPSS statistics version 21.0. Thirty-one wards were aggregated into three main specialities: medicine (including: internal medicine, oncology, haematology, nephrology, gastroenterology, neurology, cardiology, pulmonology, urology, gynaecology, paediatrics and geriatrics), surgery (including: neurosurgery, orthopaedics, cardiothoracic surgery, surgery, otorhinolaryngology, oral surgery, and obstetrics), and intensive care units (ICU) (including: intensive and medium care, and neonatal intensive care).
Standard frequency tabs were used to present the main results and antibiotics are presented at the WHO ATC-5 level.6 Continuous variables are expressed as proportions. Categorical variables are expressed as proportions and were analysed by Fisher’s exact test or Pearson’s chi-square test where applicable. Logistic regression analysis was performed in order to determine whether or not a variable was associated with guideline compliance or rate of consulting an IDS. Univariable logistic regression analysis was used to assess the relationship of each potential predictor with the outcome measure. Variables were included in the multivariable logistic regression analysis based on a p-value ≤ 0.25 in the univariable analysis. Using a backward and a stepwise forward approach for the iterative process of variable selection, variables were removed from the model if they were considered not statistically significant at a p-value ≤ 0.05. The probability of effect modification was controlled by adding interaction terms to the multivariable logistic regression analysis. A variable was considered to be an effect modifier when the interaction term turned out to be significant at p ≤ 0.1. The predicting accuracy and variation of the models was estimated by using the Hosmer and Lemeshow test and the Nagelkerke Pseudo R2 . For the Hosmer and Lemeshow test, poor fit was indicated by p < 0.05. The Nagelkerke Pseudo R2 provides an indication of the amount of variation in the dependent variable explained by the model; since we used many questionnaires, a variation percentage < 10% was considered as low.
RESULTS
Overview of prescribing
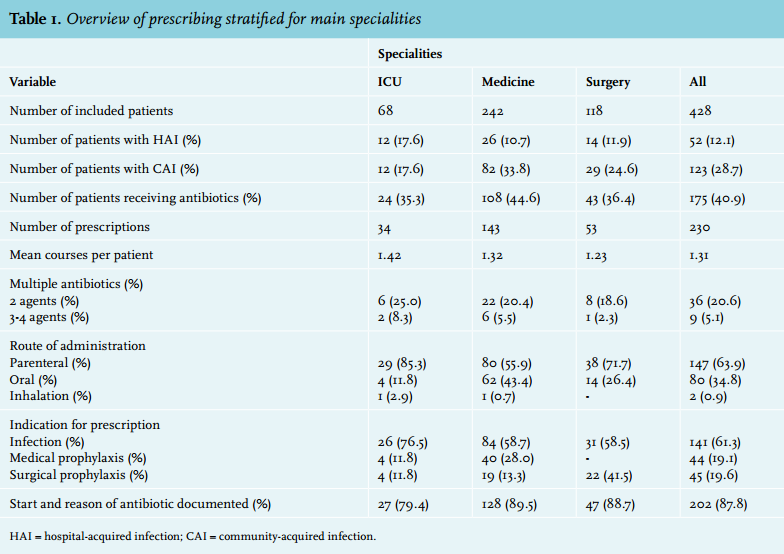
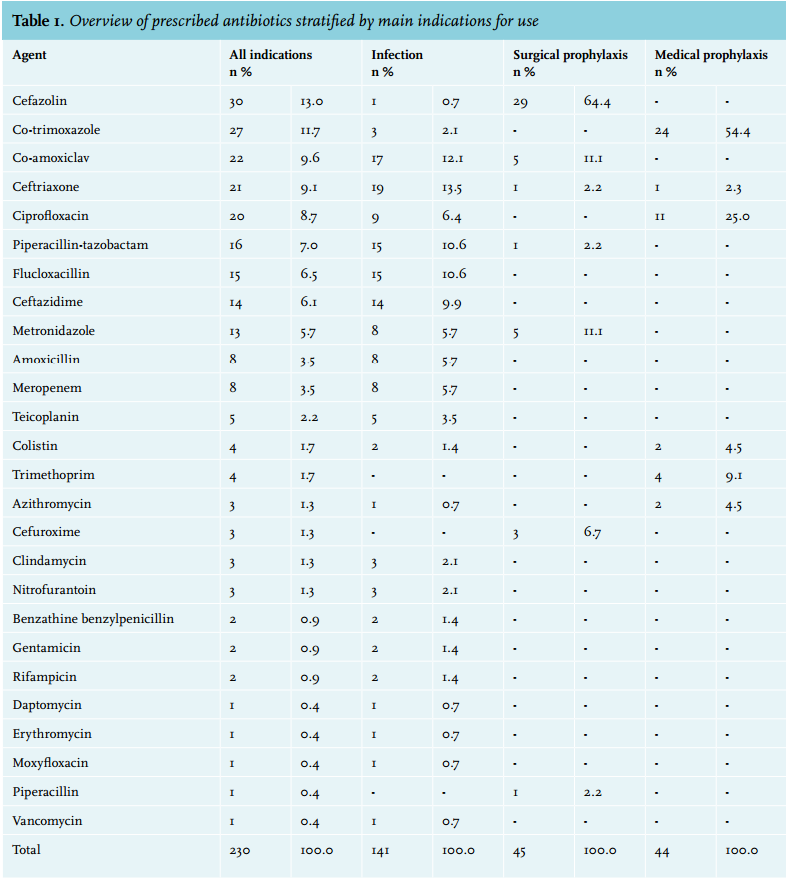
A total of 428 hospitalised patients were evaluated, of whom 175 (40.9%) were prescribed 230 antibiotics, representing 1.31 courses per patient. More than one agent was prescribed to 25.7% of all patients who were on antibiotics. Data for proportions of treated patients, proportion of patients receiving multiple antibiotics, parenteral route of administration, inclusion of start and reason in patient record for the different main specialities are summarised in table 1. Overall, 63.9% of antibiotics were administered via the parenteral route. Large differences in the proportion of parenteral use were found among departments, with a significantly higher intravenous rate (p = 0.001) in the ICU (85.3%) compared with medical (55.9%) and surgery (71.7%) departments. The reason was documented in medical records for the majority (87.8%) of antibiotic prescriptions. There was no significant difference in documentation rate between specialities. However, the documentation rate was associated with the indication for prescription of antibiotics. Surgical prophylaxis had a significantly higher documentation rate (100%, p = 0.01), compared with medical prophylaxis (79.5%) and therapeutic antibiotics (86.5%). Of the 141 prescriptions that concerned antibiotics for therapeutic use, 70.2% (n = 99) were prescribed for empirical therapy, of which 29.3% (n = 29) were prolonged after 72 hours of treatment in the presence of a negative culture result, or in the absence of culture samples. Only 42 prescriptions were directed at a known pathogen. The top 5 sites of infection accounted for > 60% of all therapeutic prescriptions. Respiratory tract infections (RTI) (18.4%; n = 26) and skin, soft tissue, bone and joint infections (18.4%; n = 26) were most common. Other common infections were urinary tract infections (12.8%; n = 18), infections of the central nervous system (8.5%; n = 12), and intra-abdominal infections (7.8%; n = 11). Forty-five prescriptions were for surgical prophylaxis, of which 6.7% (n = 3) were prolonged for more than 1 day. Forty-four prescriptions were issued for medical prophylaxis, mainly for haematology and oncology patients. An overview of the antibiotics prescribed, stratified for indications, can be found in the supplementary data.
Guideline compliance
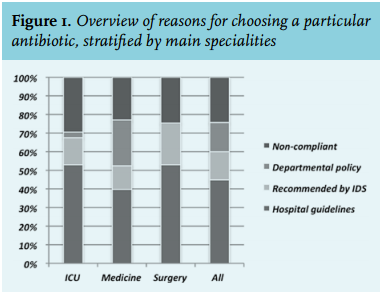
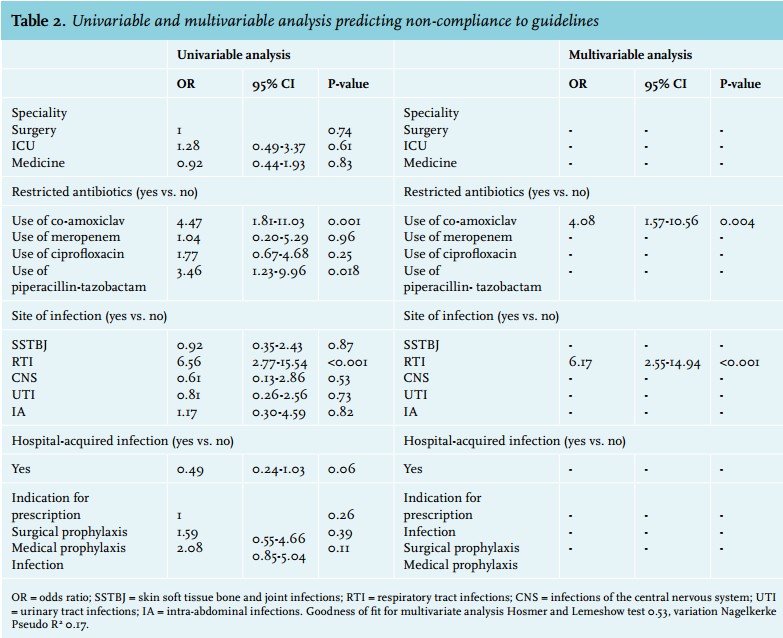
Guideline compliance was calculated by the sum of prescriptions compliant with hospital guidelines (44.8%), prescriptions according to departmental guidelines which are not approved by the hospital antibiotic committee (15.7%) and prescriptions recommended by an IDS (15.2%), resulting in an overall compliance rate of 75.7%. Medicine departments prescribed significantly more often according to guidelines used on wards (p < 0.001) compared with surgical departments and the ICU. No differences between the main specialities were found for prescribing according to hospital guidelines or based on the recommendations of an IDS. Figure 1 presents an overview of reasons for choosing a particular antibiotic stratified by main specialities. Table 2 shows an overview of the univariable regression analysis including all potential predictors assessed, and the final multivariable regression analysis predicting non-compliance to guidelines. The strongest predictor for non-compliance was RTI (26 prescriptions were indicated for RTI, non-compliance 61.5%, crude OR 6.56, 95% CI 2.77-15.54, OR adjusted for amoxicillin/clavulanic acid 6.17, 95% CI 2.55-14.94). Prescription of amoxicillin/clavulanic acid (22 prescriptions, non-compliance 54.5%, five amoxicillin/clavulanic acid prescriptions were indicated for RTI, non-compliance 60.0%), recorded an OR of 4.08 (95% CI 1.57-10.56). Further analysis of data did not reveal an association between the use of amoxicillin/clavulanic acid and treatment of RTI for any specific speciality (data not shown).
Consultation of infectious disease specialist
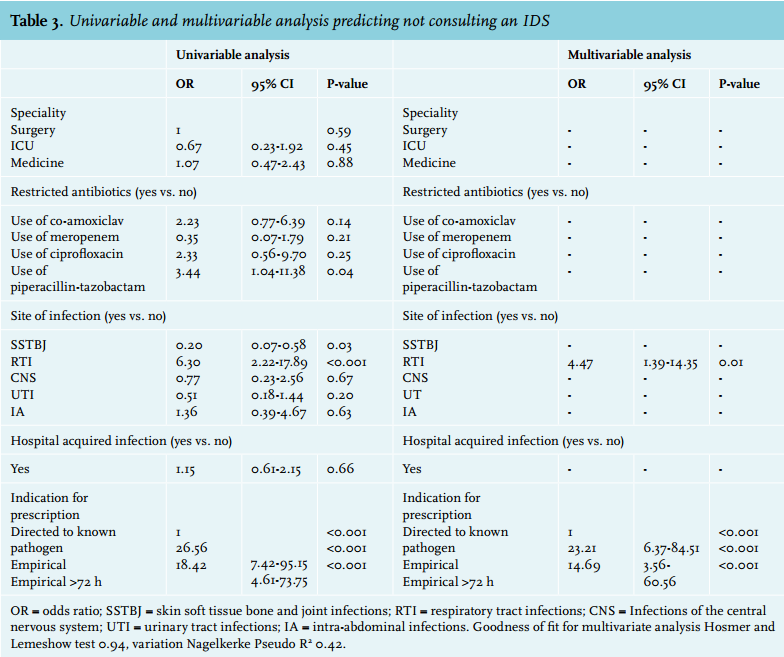
An IDS was involved in 76 (33.0%) of all prescriptions for antibiotic therapy, mainly in response to culture results (n = 49; 64.5%). No significant differences in consulting rate were found between the three main specialities. Table 3 shows an overview of the univariable regression analysis including all potential predictors assessed, and the multivariable regression analysis predicting not consulting an IDS. Indication for prescription was the strongest predictor for consulting an IDS. Physicians less often consulted an IDS for empirical therapy (OR 23.21; 95% CI 6.37-84.51) or prolonged empirical therapy (OR 14.69; 95% CI 3.56-60.56) compared with consultation for prescriptions that were based on culture results. In addition, fewer consultations were requested for RTI (OR 4.47; 95% CI 1.39-14.35).
Time investment
Data were collected by a multidisciplinary team of 15 persons, with an average time investment of 1.5 hours per person. Because of the advanced electronic patient records used by Radboudumc it was possible to see at a glance whether or not a patient was on antibiotics. In addition, practically all information could be found in the patient records. If, accidentally, the reason for prescription was not documented or if the reason for antibiotic choice was not according to hospital guidelines or on advice of an IDS, the attending physician was consulted by the team member during their weekly consultation at the department. Preparation ahead of the PPS, writing a protocol and developing registration forms both tailored to the hospital, instruction for data collection team, time needed for planning and informing departments was estimated at 16 hours. Time required for data preparation and data analysis took a further estimated 16 hours.
DISCUSSION
This PPS provides a clear overview of total antibiotic use and the indications for prescriptions in a tertiary care centre. Of 428 patients included, 40.9% received antibiotics, which is in line with recent prevalences reported for other Dutch tertiary care hospitals.7 The overall guideline compliance in this study was 75.7%, and amongst the highest reported by other studies in the field (range 52.4-70.0%).8-10 However, there was a wide range in compliance rate between departments.
Several targets for improving the quality of antibiotic use were identified in this study. The low guideline compliance for the treatment of RTI was surprising, in particular the high use of amoxicillin/clavulanic acid. The low rate of consulting an IDS in case of RTI may explain this, and at the same time indicates a mode for improvement. This applies to prescribing empirical therapy for > 72 hours in the presence of a negative culture result or in the absence of culture samples obtained, even though, with this definition, a few patients (e.g. patients with communityacquired pneumonia who cannot produce sputum) might be misclassified. This should be analysed in more depth in future surveys. The deviation from hospital guidelines and frequent use of departmental protocols in oncology and haematology departments is remarkable and another target for intervention, either to integrate in hospital general guidelines as far as these protocols are evidence-based or otherwise to exclude from further use. The fact that the use of amoxicillin/clavulanic acid was significantly associated with low guideline compliance might indicate that additional measures, such as pre-authorisation or post-prescription review, are desirable. It has been demonstrated that non-guideline compliance often leads to the use of more broad-spectrum antibiotics.11 Prescribers should be more aware that a more broad-spectrum empirical therapy does not result in more effective treatment, but does increase the selection of antibiotic resistance. Empirical therapy should be de-escalated to culture results whenever possible. The large number of empirical therapies that were not de-escalated within 72 hours, when culture results became available, is another area with room for improvement. In these cases, it was less likely that an IDS had been consulted, and such consultation may help to improve outcome.
The overall percentage of hospital-acquired infection (HAI) reported in this survey (12.7%) is higher than percentages reported for tertiary care hospitals in other European studies (range 4.0%-9.7%).5,7 As expected, the ICU had the highest proportion of patients treated for HAI. However, 22% of all patients with HAI were transferred from other hospitals and might have acquired the infection earlier. Therefore, the prevalence of HAI in a tertiary care hospital may not necessarily reflect the local risk of infection.
Overall, and as reported in other European and national studies, b-lactams are the most frequently prescribed class of antibiotics.10,12 The use of combinations of penicillins with enzyme inhibitors, third-generation cephalosporins, fluoroquinolones and carbapenems was found to be in line with the proportions reported for university hospitals in Nethmap 2013, the national surveillance report on antimicrobial use and resistance in the Netherlands.12 For 87.8% of cases, the reason for prescription was documented, which was found to be in line with documentation rates reported in other European studies (range 27.2%-92.3%).9,10,13,14 However, these numbers indicate that there is still room for improvement. Documentation of start and reasons in the patient record is associated with more appropriate antibiotic prescribing,15,16 and therefore, ECDC has identified this parameter as a key performance indicator.5
This study has several weaknesses. First, as in any PPS, this study was cross-sectional and thus only presents a snapshot of prescribing. Therefore, repeated PPS or follow-ups are necessary in order to identify patterns in prescriptions, seasonal variation and to assess changes in prescribing behaviour. Secondly, based on the data collected, no statement could be made on whether or not patients who received parenteral antibiotics where eligible for a parenteral-oral switch of antibiotics. It is therefore recommended for future studies to add the item whether or not a patient is eligible for a parenteral-oral switch at the moment of the PPS.
In conclusion, the present study revealed several areas of practice that deserve specific attention in an institutional antimicrobial stewardship program. The most important targets identified are the low guideline compliance rate for amoxicillin/clavulanic acid and RTI, the frequent use of departmental protocols other than hospital antibiotic guidelines, and the large number of prescriptions for RTI and for prolonged empirical therapy without consulting an IDS. Despite the fact that a PPS only presents a snapshot of prescribing, it is helpful in setting priorities for quality improvement of antibiotic prescribing. Repeated PPS are necessary to reveal patterns in antibiotic prescribing and to evaluate the effectiveness of interventions, and it is recommended to perform a PPS at least once a year.
ACKNOWLEDGMENTS
The authors thank E. Kolwijck, I. Maat, S. Debaest, J. van Ingen, I. Lede, J. van Pelt, B. Lestrade, R. van Crevel, B. Rodenburg, J. Kleinnijenhuis, R. Brüggemann, E. van der Wouden, N. van Erp, E. Muilwijk, B. Jacobs, K. de Kanter for their participation in data collection and T. Sprong, Canisius Wilhelmina Hospital, Nijmegen for his assistance in setting up the PPS.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES
SUPPLEMENTARY DATA
Detailed description of data collection
Standardised case record forms were used for data collection, which included details on the number of inpatients in each department, patient age and gender, surgery in the past 30 days, transfers from other hospitals or nursing homes, antibiotics prescribed, route of administration, indication for prescribing (i.e. empirical, prolonged empirical (> 72 hours), medical prophylaxis or surgical prophylaxis), type of infection (i.e. hospital-acquired infection (HAI) or community-acquired infection (CAI)), site of infection, adherence to guidelines, documentation of reason for prescription in notes, and documented consultation of an infectious disease specialist (IDS).
The term ‘prescription’ was used to indicate every time an individual antibiotic was prescribed. Prescriptions were defined as either prophylactic or therapeutic. Antibiotics prescribed without clinical evidence of infection, and without a statement in the electronic patient record indicating a specific suspected infection were considered prophylaxis.1 Prophylactic antibiotics were defined as a prescription in order to prevent the patient from acquiring an infection, and could either be surgical prophylaxis to prevent postoperative infections, or medical prophylaxis to prevent infections in the immunocompromised patient. Antibiotic therapy, prescribed before culture results were known, was considered to be empiric therapy. Empiric therapy used > 72 hours in the presence of a negative culture result or in the absence of culture samples was defined as prolonged empiric therapy.1
In the Radboudumc, restricted release of antimicrobial agents has been implemented as a method to improve antibiotic prescription. The restricted-release antibiotics include piperacillin-tazobactam, carbapenems, thirdand fourth-generation cephalosporins, glycolpeptides and aminoglycosides. At the time of the study, the Radboudumc antibiotic committee considered adding amoxicillin-clavulanic acid (co-amoxyclav) to this list of restricted release antibiotics.
Consultation by an IDS was classified as: (I) initiated by the IDS in response to culture results, (II) initiated by the attending physician in response to culture results, (III) initiated by the attending physician, not in response to culture results.
Infections could be either a hospital-acquired or a community-acquired infection. CAI were defined as cases where symptoms or antibiotics were started < 48 hours after a patient was admitted or > 30 days after discharge or surgery, while HAI were defined as cases where symptoms started > 48 hours after admission to hospital or < 30 days after surgery or discharge.2 HAI were classified into four categories: (I) post-intervention (e.g. ventilator-associated pneumonia, intravenous catheter or urinary catheter), (II) postoperative, (III) Clostridium difficile-associated diarrhoea, and (IV) other HAI.
REFERENCES