CASE REPORT
A 68-year-old woman presented with a purple lesion on her finger. She had diabetes type 2 and kidney failure due to atherosclerotic vascular disease, and had undergone a kidney transplantation two months earlier. The skin lesion started as a small blister after mild trauma, developing into a blue spot on the tip of the left index finger. This resolved spontaneously, but after six weeks multiple small, painful vesicles and a purple papule arose again. Her immunosuppressive treatment consisted of tacrolimus, prednisolone and mycophenolate mofetil. Her diabetes was treated with insulin therapy. She did not smoke, drink, or abuse any kind of drugs. On physical examination there were a few clear-pale lenticular vesicles on the distal phalanx of the finger and on top a blue-purple papule with a haemorrhagic crust (figure 1). The finger was warm, arterial pulsations on the left arm were normal and she did not have any fever. Laboratory results showed a stable serum creatinine, and normal levels of calcium, phosphate and thrombocytes.

DIAGNOSIS
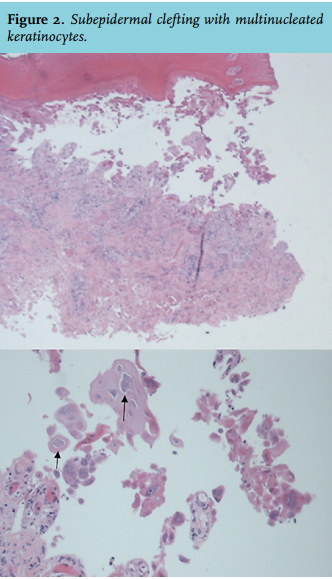
The differential diagnosis of a black or purple coloured finger is: vascular obstruction (microangiopathy, vasculitis, septic or cholesterol embolism), calciphylaxis, malignancy (melanoma, paraneoplastic tumour thrombi) or local infection (bacterial or viral). A skin biopsy showed subepidermal clefting with several multinucleated keratinocytes and a ground glass appearance of the nuclei (figure 2). There was a perivascular mononuclear cell infiltrate in the dermis without signs of micro-angiopathy or thrombi. The histology was characteristic for a herpes infection, which was confirmed by a positive polymerase chain reaction for herpes simplex virus (HSV) type 1.
The patient told us that she had had a cold sore a few weeks before, which was probably the source of the herpes infection of the finger. A HSV infection involving the hand is called herpetic whitlow.1 The infection can be caused by HSV type 1 (usually presenting as gingivostomatitis) or type 2 (mostly presenting as genital herpes).2 Direct contact of the finger with secretions or lesions of infected areas is the likely mechanism of transmission. It is especially seen in young children (finger sucking), dentists, young adolescents, and immunocompromised patients.3 Classically, a single vesicle or a cluster of vesicles arises near the nail, 3-4 days after skin irritation or minor trauma. Vesicles are first clear-pale yellow, and later become turbid or haemorrhagic. Most patients have intense localised pain. The lesion might resemble a felon (also called whitlow).1,4 The natural course is usually benign with complete resolution within 2-3 weeks. Systemic viraemia or ocular infection are rare, but severe, complications. After resolution of the infection, the herpes virus passes into a latency phase, inhabiting a host neural ganglion. One or more recurrences are experienced in 20-50% of patients and usually arise in the same dermatome as the original infection. Immunocompromised patients are at greater risk of more frequent and more severe HSV recurrences. The diagnosis is usually made on clinical grounds, but may be confirmed with polymerase chain reaction or immunofluorescence microscopy in which scrapings of the lesions are examined for herpes antigens.1,4
Treatment is symptomatic, but antiviral drug therapy can be beneficial. Acyclovir seems to prevent or decrease recurrence rates. Intravenous acyclovir is occasionally required in cases of immunosuppression and disseminated HSV infection.1 We started valacyclovir orally, after which the patient recovered fully.
REFERENCES
1. Rubright JH, Shafritz AB. The Herpetic Whitlow. J Hand Surg Am. 2011;36:340-2.
2. Gill MJ, Arlette J, Buchan K. Herpes simplex virus infection of the hand. A profile of 79 cases.
Am J Med. 1988;84:89-93.
3. Wu IB, Schwartz RA. Herpetic whitlow. Cutis. 2007;79:193-6.
4. Clark DC. Common acute hand infections. Am Fam Phys. 2003;68:2167-76.