KEYWORDS
Bacterial meningitis, S. pneumoniae, risk factors, predisposing factors
INTRODUCTION
Bacterial meningitis is a life-threatening infection of the central nervous system.1 Streptococcus pneumoniae and Neisseria meningitidis are the leading causative organisms, with the first being responsible for two-thirds of the cases in Western Europe and the United States.2,3 Mortality is approximately 20% in high-income countries despite available treatment with antibiotics and dexamethasone, and is several times higher in low-income countries.4,5 Approximately half of the survivors have neurological sequelae such as hearing impairment, focal motor deficits or cognitive impairment.6
Invasive disease by pneumococci and meningococci ispreceded by nasopharyngeal colonisation. Asymptomatic colonisation of pneumococci and meningococci occurs in up to 100% and 18%, respectively, of the normal population.7 In some persons these common colonisers are able to breach the mucosal barrier, survive in the blood stream and cross the blood-brain barrier to cause meningitis. Several factors have been identified that increase the susceptibility for bacterial meningitis. These can consist of specific age groups, medical conditions that cause immunodeficiency, host genetic factors and anatomical defects of the natural barriers of the central nervous system. 2 Patients with underlying conditions generally have a higher risk of having a poor outcome, and therefore identification of these groups and preventive measures such as vaccination are of the utmost importance (table 1).
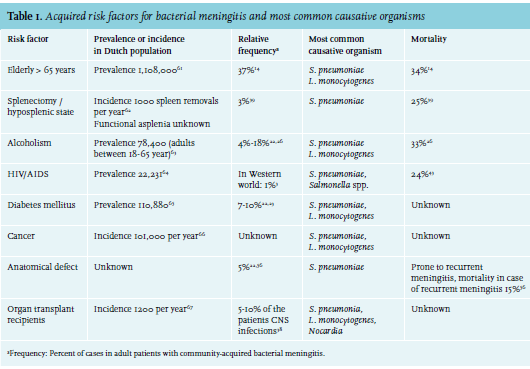
Pneumococcal disease including meningitis is seen mostly in children below 2 years of age or adults over 50 years. Furthermore, susceptibility is increased in individuals with underlying conditions such as splenectomy or asplenic states and in children with cochlear implants. The use of immunosuppressive drugs, the presence of diabetes mellitus, a history of splenectomy, infection with HIV or alcoholism is found in 20% of adults with pneumococcal meningitis.2 HIV infection affects the aetiology of acute meningitis, and is especially important in lower-income countries.4 The meningococcus is the leading pathogen of meningitis in young children beyond the neonatal period and in young adults. Meningococcal disease has been associated with smoking, living in the same household as a patient (including students), and meningococcal disease in proxies.8 Defects in innate immunity have been described to be associated with susceptibility to both pneumococcal and meningococcal infections within families.2 In this review we describe risk factors for community-acquired bacterial meningitis, preventive measurements and treatment options.
AGE
The incidence of meningitis is highest in young children and the elderly.9 In infants the waning passive immunity acquired from the mother and immature own immune system results in an increased susceptibility to bacterial infections. Due to the introduction of conjugated vaccines against Haemophilus influenzae type B and S. pneumonia, infants have become protected against these infections, and the age distribution of bacterial meningitis patients subsequently shifted. Whereas previously bacterial meningitis was mostly a disease of children and adolescents, currently most patients are elderly with an average age of 50.3 In children, the common causative organisms have changed as a result of vaccinations, but clinical characteristics have not. Young infants with bacterial meningitis can present with nonspecific signs such as lethargy, poor feeding or irritability. Older children are more likely to present with typical signs and symptoms of bacterial meningitis.3 The most common causative organisms are S. pneumoniae and N. meningitidis in infants older than one month (80% of cases in the Netherlands).10 The remainder of cases is caused by group B streptococci, E. coli, H. influenzae, other Gram-negative bacilli, L. monocytogenes and group A streptococci. Recommended treatment consists of a third-generation cephalosporin (cefotaxime or ceftriaxone).10 A meta-analysis of randomised trials showed a beneficial effect of dexamethasone in children in high-income countries in respect to hearing loss; in low-income counties this was not established.2
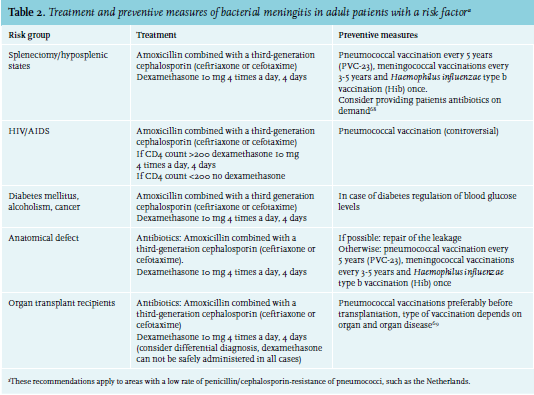
In the elderly, the function of the immune system declines, which has also been referred to as ‘immunosenescence’.11 Immunosenescence leads to increased susceptibility to infections in elderly patients, but also to reduced vaccine efficacy, and possibly autoimmune disease and cancer.12,13 Elderly patients also frequently have comorbid conditions that affect the immune system. Symptoms can be atypical, and neck stiffness and headache are less frequently present, while focal neurological abnormalities occur more often.2 The spectrum of causative bacteria is slightly different from younger adults, as L. monocytogenes is more frequently identified.14 Vaccination of elderly patients with pneumococcal vaccines is currently not recommended in Dutch national guidelines because of a lack of evidence of effectiveness in the elderly.15 Recommended treatment consists of ceftriaxone and amoxicillin (to cover for L. monocytogenes) in combination with adjunctive dexamethasone (table 2).
IMMUNODEFICIENCY
Life expectancy has increased due to advances of medical science and technology, and diseases that were previously uniformly lethal have now become chronic illnesses.16,17 As a result, the number of immunocompromised individuals has increased over the past decades. Half of the patients with bacterial meningitis have predisposing conditions, one-third of these patients have an immunodeficiency.3 Splenectomy, alcoholism, HIV, diabetes mellitus, cancer or the use of immunosuppressive medications have been recognised as risk factors for invasive bacterial infections including meningitis.2 The most common causative organism of bacterial meningitis in patients with an immunocompromised state is S. pneumoniae, although other causative organisms may also be encountered in patients with specific risk factors.2,3,18
Diabetes mellitus
Diabetes mellitus has been reported as a risk factor for bacterial infections, and infection is an important cause of mortality in diabetic patients.19-21 In reports of community-acquired bacterial meningitis in adults, diabetes was present before admission in 7-10%.22,23
Common pathogens in diabetic patients with meningitis are S. pneumoniae and L. monocytogenes.18,22,23 As diabetes is a risk factor for invasive pneumococcal disease in general, physicians in the United States and some European countries are advised to vaccinate diabetic patients with the 23-valent polysaccharide pneumococcal vaccine.24 A large proportion of patients with bacterial meningitis are hyperglycaemic on admission, also of those without diabetes.23 In these patients, high blood glucose levels are probably an epiphenomenon of severe illness. Blood glucose levels should be managed, although treatmentrelated hypoglycaemia should be avoided. Hypoglycaemia in bacterial meningitis is associated with unfavourable outcome and increased risk of major complications such as seizures and brain damage.23 Adjunctive treatment with dexamethasone can cause further dysregulation of blood glucose levels,25 so follow-up of blood glucose concentrations in all bacterial meningitis patients is warranted.
Alcoholism
Excessive alcohol use results in increased susceptibility to infections, probably due to a decreased innate and adaptive immune response.26 It is unclear if alcoholism is an independent risk factor for bacterial meningitis. Patients who suffer from alcoholism have worse general health, are more prone to head injury and more often have chronic liver disease,26-28 all factors that have been associated with increased risk of bacterial meningitis. In a prospective nationwide observational cohort study of 696 episodes of bacterial meningitis, 4% of the patients were alcoholics.26 Twenty-five patients with alcoholism suffered from a second episode of meningitis during this study, suggesting an association between alcoholism and bacterial meningitis, although a causal relationship remains unclear due to comorbid conditions. The most common causative organisms of bacterial meningitis in alcoholic patients were S. pneumoniae (70%) and Listeria monocytogenes (19%).26 Alcoholics had a higher rate of complications compared with non-alcoholic patients (81% vs. 62%) and a higher rate of unfavourable outcome (67% vs. 33%). Complications most often consisted of cardiorespiratory failure due to underlying pneumonia or endocarditis. In a recent study, patients with bacterial meningitis and endocarditis were more often found to be alcoholics (17% vs. 4% in bacterial meningitis patients without endocarditis) and sometimes presented with the Austrian syndrome, consisting of pneumococcal meningitis, pneumonia and endocarditis.29 Prognosis in these patients is generally poor.29 Treatment should consist of amoxicillin and a third-generation cephalosporin combined with dexamethasone (table 2).
Cancer
Patients with cancer are more susceptible to infections for several reasons;30 the disease itself can predispose to infections (especially haematological malignancies such as multiple myeloma) as does treatment with immunosuppressive chemotherapy, malnutrition and presence of indwelling venous catheters.30-32 Patients with cancer were also found to have an attenuated inflammatory response in the central nervous system.33
Susceptibility for meningitis is particularly increased in patients with leukaemia and lymphoma; one-fourth of all central nervous system infections in cancer patients are found in this group. Patients with cancer who recently underwent neurosurgery are also at risk for meningitis; these patients account for 75% of the meningitis cases in cancer patients.34 In a retrospective study in 77 patients with cancer, S. pneumoniae was t he most common causative organism; other relatively frequent causative organisms included
L. monocytogenes and Cryptococcus neoformans. Only 57% of these patients had cerebrospinal fluid (CSF) pleocytosis, reflecting the immunocompromised state of cancer patients.33 Infections in these patients may go undetected because signs and symptoms can be atypical, resulting in a possible delay to diagnosis and treatment.31,34 Another cause of diagnostic delay is deferral of lumbar puncture because of thrombocytopenia or intracranial space occupying lesions.35 In high-risk cancer patients who are severely immunocompromised, vaccination or even prophylactic antibiotic treatment may be warranted.
Organ transplant recipients
Invasive pneumococcal infections occur more frequently in organ transplant recipients because of treatment with immunosuppressive therapy to prevent and treat rejection of the graft.36 Liver transplant recipients have the highest incidence (354 per 100,000 persons per year), possibly due to a higher incidence of additional malfunction of the spleen. Time of onset of invasive pneumococcal disease after organ transplant is variable and the risk persists over time.37 Other causative organisms include Nocardia (especially in case of multiple brain abscesses) and Listeria monocytogenes.38 In organ transplant receivers with suspected bacterial meningitis, the differential diagnosis may include cryptococcal, tuberculous or other uncommon types of meningitis, in which adjunctive dexamethasone may be harmful without proper antibiotic coverage. Therefore, when bacterial meningitis is suspected in transplant patients, the potential benefit of adjunctive dexamethasone should be weighed against the risk of deterioration when it is caused by uncommon pathogens. The risk of invasive pneumococcal infections can be decreased by pneumococcal vaccination prior to transplantation. Administration of prophylactic antibiotics in these patients remains controversial, as there is a risk of resistance and recommendations in current guidelines vary.37
Splenectomy or hyposplenic state
Dysfunction or absence of the spleen predisposes to infections with encapsulated bacteria such as S. pneumoniae and Haemophilus influenzae.39 A hyposplenic state can be congenital or acquired after surgical removal of the spleen (splenectomy). Furthermore, acquired functional hyposplenism occurs in 15-40% of the cases after allogeneic bone marrow transplantation and other causes of hyposplenism are graft-versus-host disease, sickle-cell anaemia, celiac disease and HIV infection.40 The spleen is the only site in the human body where poorly opsonised bacteria such as S. pneumoniae can be cleared from the bloodstream and therefore hyposplenic patients are at risk for overwhelming sepsis caused by these bacteria.39 Although this risk has been recognised for almost a century,43 patients still do not receive adequate vaccination or information from their physicians about their risk of infection and when to seek medical attention.39 S plenectomy or functional hyposplenia is an uncommon risk factor for bacterial meningitis and was identified in 24 of 965 cases (2.5%) of communityacquired meningitis in a prospective nationwide cohort study, and was associated with a high rate of mortality (25%) and unfavourable outcome (58%). In this cohort study, all cases in patients with hyposplenia or asplenia were caused by S. pneumoniae. The increased risk of infections by encapsulated bacteria is life-long, and the median time between splenectomy or diagnosis of functional hyposplenia and the bacterial meningitis episode was found to be 16 years, with a range from 1-54 years.39 In the majority of cases current guidelines for prevention of infection were not adhered to.39,42 Preventive measurements such as sufficient and repeated vaccinations, patient education on how to recognise meningitis, and prescription of prophylactic antibiotics could be used to reduce the number of cases of bacterial meningitis in these individuals.39,42
HIV/AIDS
HIV-infected individuals have a 6- to 324-fold increased susceptibility for invasive pneumococcal disease.2 The increased susceptibility is caused by a decreased humoral immunity: B-cell activation is impaired, resulting in decreased IgM synthesis and both T-cell dependent and T-cell independent differentiation of B-cells is impaired.43 This results in a decreased humoral response to bacteria. In more advanced stages of HIV these disturbances are more pronounced and therefore most episodes of bacterial meningitis occur in individuals with a CD4 cell count of less than 200 cells per cubic millimetre.43 Most of these patients are severely immunocompromised and do not take antiviral therapy. The most common causative bacterial agent of bacterial meningitis in HIV-infected individuals is
S. pneumoniae, but Salmonella meningitis also occurs more frequently compared with HIV-negative controls.2 In case of low CD4 counts, the differential diagnosis of bacterial meningitis is broad; tuberculous meningitis, cryptococcal meningitis and toxoplasma meningoencephalitis should be considered.
Ninety percent of the worldwide HIV-infected individuals live in low-income countries and bacterial meningitis is at least ten times more common in these regions. Diagnosis of bacterial meningitis in patients with HIV can be extremely difficult in resource-poor settings, with no imaging available and limited laboratory facilities.4 Furthermore, antibiotic resistance and partially treated bacterial meningitis is an increasing problem in Africa, where antibiotics are often sold ‘over the counter’; approximately 5% of the S. pneumoniae isolates have reduced susceptibility to ceftriaxone.4
A prospective cohort study in Spain performed in 2009 showed that there are several differences between HIV-infected and HIV-negative meningitis patients in high resource settings.43 In this study 32 episodes of bacterial meningitis in HIV-infected patients were compared with 267 episodes in HIV-negative patients. HIV-infected patients with bacterial meningitis presented with more severe disease, reflected by a higher rate of altered mental state, focal neurological deficits and concomitant pneumonia. Leukocyte counts in the CSF were lower in HIV-infected patients, probably reflecting an impaired immune response.43 In the United States national guidelines advise pneumococcal vaccinations in HIV-infected individuals.44 Because of a presumed low prevalence of pneumococcal infections in patients with HIV in the Netherlands, Dutch national guidelines only advise pneumococcal vaccination in case of concomitant use of intravenous drugs and state that in other HIV-infected individuals vaccination can be considered.15 Studies that assessed vaccine efficacy of pneumococcal vaccinations in case of HIV infection have varying and conflicting results.45 HIV-infected patients with CD4+ T-lymphocyte counts less than 500 cells/ul often have lower responses to pneumococcal vaccination.44 Despite these uncertainties, vaccination is considered safe in this risk group and as the potential benefit is substantial, vaccination is advised.46,47
HOST GENETIC SUSCEPTIBILITY
The risk of acquiring bacterial infections is largely heritable, as shown by family, twin and adoption studies.7,48 Several genetic traits for developing meningococcal and pneumococcal disease have previously been described in extreme phenotype studies, of which most concerned genetic deficits in genes coding for complement system proteins.7 An increased incidence of invasive meningococcal meningitis was found in patients with a properdin deficiency and with deficiencies in the complement system (C5, C6, C7, C8 and, possibly, C9) in extreme phenotype studies.2 A review and meta-analysis of genetic risk factors for invasive pneumococcal and meningococcal disease showed genetic variation in NFKBIA, NFKBIE, and TIRAP genes was protective, whereas PTPN22 and MBL2 variants were associated with increased susceptibility for pneumococcal disease.7 Increased susceptibility to invasive meningococcal disease was associated with genetic variants in the CFH, SFTPA2, CEACAM3, and CEACAM6 genes, whereas other CEACAM6 and SFTPA2 variants showed a protective effect.7
Recently, studies have addressed specific genetic risk factors for bacterial meningitis.25,49-51 A genetic association study in adult bacterial meningitis patients showed that a common single nucleotide polymorphism (SNP), the complement factor 3 gene (C3), was associated with susceptibility for bacterial meningitis (OR 4.50, 95% CI 1.62-12.50).49 Interestingly, the protective genotype of this SNP was previously shown to increase the risk of age-related macular degeneration, showing that a more readily activated complement system may protect against bacterial infection while simultaneously increasing the risk of autoimmune disease. In the same cohort, polymorphisms in mannose binding lectin (MBL2) resulting in MBL deficiency were shown to increase the risk of pneumococcal meningitis.52 Patients homozygous for variant alleles in exon1 of MBL2 had eightfold (OR 8.21, 95% CI 1.05-64.1) increased susceptibility for pneumococcal meningitis. Also, high CSF MBL levels were associated with poor disease outcome and increased disease severity, suggesting that the lectin pathway is a possible target for adjunctive therapy in pneumococcal meningitis.52
After an experimental meningitis model showed N. meningitidis passes the blood-brain barrier by using the beta2-adrenoceptor,53 genetic variation in the gene coding for this receptor (ADRB2) was shown to influence the risk of bacterial meningitis (OR 1.35, 95% CI 1.04-1.76).54 Non-selective beta-blockers down-regulate this receptor, and therefore could be tested as a target in experimental studies to see whether it may decrease susceptibility to bacterial meningitis.54
Two studies from a Dutch paediatric cohort showed that susceptibility to bacterial meningitis was associated with genetic polymorphisms in Toll-like receptor (TLR) 2, 4, and 9 and nucleotide oligomerisation domain-like receptor 2.50,51 TLRs and nucleotide polygomerisation domain-like receptors (NODs) are pathogen-recognising receptors and SNPs in genes coding for these receptors are thought to influence susceptibility, but also disease severity and outcome of bacterial meningitis by altering the inflammatory response.50,51 TLR4 and NOD2 SNPs were significantly associated with susceptibility to meningococcal meningitis in children, and carriage of a combination of the risk alleles in TLR2/TLR4 and TLR4/NOD2 SNPs showed an even stronger association.51 TLR9 SNPs were associated with a reduced susceptibility to meningococcal meningitis in this study.50 Identification of genetic risk factors for bacterial meningitis may be used in future studies to identify pathophysiological mechanisms and could change vaccination policy in patients with established genetic risk factors.
ANATOMICAL DEFECTS
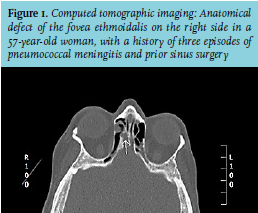
The blood-brain barrier separates the central nervous system from the circulation and is an important defence mechanism against bacteria invading the central nervous system. It also maintains a stable environment inside the nervous system and potentiates molecular transport between blood and brain. Disruption of this barrier can occur following trauma, surgery, congenital defects or ear and sinus infection and provides an entry for bacteria.55 When a patient has recurrent episodes of bacterial meningitis a disruption of the blood-brain barrier should be suspected, especially when the causative organism is S. pneumonia, but also N. meningitides, S. aureus and H. influenzae are possible causative organisms in case of a CSF leak.56 With atypical causative organisms, or recurrent meningococcal meningitis, an immunodeficiency (e.g. complement or properdin deficiency) should be suspected. When no apparent cause of recurrent meningitis is identified on clinical grounds, diagnostic procedures should be performed to identify anatomical defects because of the high prevalence of this cause of recurrent meningitis (figure 1).56 Optimal imaging consists of thin-slice CT of the skull base combined with MRI-3D constructive interference in steady-state imaging. It is important to take into account that small bone defects on CT do not prove CSF leakage.56 Overt CSF leakage is seldom identified on presentation and most leaks resolve spontaneously within the first 24-48 hours. In case of a persistent CSF leak 7-30% of the patients develop meningitis, and this risk increases with the duration of the leakage.55 There can be a delayed onset of several years between trauma and bacterial meningitis.58-60 With an anatomical defect and/or CSF leakage present, a neurosurgeon or otolaryngologist should be consulted to evaluate the possibility of repairing the defect. Furthermore, vaccinations should be administered in case of persistent CSF leakage. Treatment with prophylactic antibiotics in these patients remains controversial but may be considered in patients with recurrent meningitis despite vaccination.56
VACCINATION AFTER BACTERIAL MENINGITIS
The risk of a recurrence of bacterial meningitis in patients with no anatomical defect or known immunodeficiency is estimated to be 1-3%.56 Most of these cases are caused by S. pneumoniae. The risk of a second meningitis episode is substantially increased compared with the risk of a first episode in the general population. Although the efficacy of pneumococcal vaccination in this population has not been studied, it appears logical to vaccinate all patients following an episode of pneumococcal meningitis, considering the substantially increased risk and lack of side effects of vaccination. This paradigm shift needs follow-up evaluation in cohorts of bacterial meningitis patients to determine whether the risk of recurrent pneumococcal disease is reduced.
CONCLUSION
Bacterial meningitis is a potentially life-threatening disease and several conditions that increase susceptibility are identified. Awareness of risk factors for meningitis may facilitate early recognition and treatment of the disease, and vaccinations can prevent cases of bacterial meningitis in various risk groups. Sufficient preventive measures in selected groups of individuals with increased risk for bacterial meningitis may reduce the number of cases.
DISCLOSURES
The authors declare no conflicts of interest. MCB is supported by a grant from the Netherlands Organization for Health Research and Development (ZonMw; NWOVeni grant 2012 [ 916.13.078]). DvdB is supported by grants from the Netherlands Organization for Health Research and Development (ZonMw; NWO-Vidi grant 2010 [016.116.358]), and the European Research Council (ERC Starting Grant 281156).
REFERENCES