INTRODUCTION
Hyperactive thyroid nodules (HTNs) are autonomous functioning thyroid adenomas (AFTN) that produce excessive amounts of thyroid hormone. About 5-10% of all palpable solitary nodules are hyperactive.1 HTNs develop slowly over a period of years, and gradually increase their contribution to overall thyroid hormone secretion as they grow. Ultimately, this leads to (subclinical) hyperthyroidism and mostly mild thyrotoxicosis for nodules < 2.5 cm, while overt thyrotoxicosis occurs in 80% of HTNs > 5 cm.1-3 The rate of progression to thyrotoxicosis in previously euthyroid patients with HTN is about 4% per year. Atrial fibrillation and progressive osteoporosis are the main complications. The risk of malignancy in an HTN is extremely low.1-3
Until recently, radioactive iodine (RAI), surgery, and anti-thyroid drugs (ATD) have been the primary treatment options for HTNs. Treatment with ATD is not recommended as first choice because recurrence of hyperthyroidism is sure to occur after discontinuation of treatment. ATDs are mainly used to temporarily stabilise patients before they receive a more permanent therapy, or in patients with limited life expectancy, and in cases where other treatment options are not feasible or contraindicated. Surgery, i.e., unilateral lobectomy, is rarely performed despite the advantage of rapid and permanent biochemical control, with euthyroidism within several days, and recurrence or persistence of hyperthyroidism in fewer than 1% of patients.4 Information about the risk of hypothyroidism after lobectomy for HTN is very limited. The weighted mean incidence of post-operative hypothyroidism after lobectomy for benign thyroid disease in general is 22% (95% confidence interval 18-27%).5 Whether similar figures are to be expected after lobectomy for HTN is currently not known. Administration of RAI is the treatment of first choice in most countries, mainly because of its non-invasive nature and high cure rates. Euthyroidism is commonly achieved within 3-6 months in 90-95% of patients and is accompanied by a mean nodule volume reduction of 30-45%.6 The most important limitation of radioactive iodine (131I) treatment is its high risk of post-irradiation hypothyroidism. Although early studies using a fixed activity of 740 MBq have reported a prevalence of 5-10%, more recent long-term studies have reported a 10-year risk of hypothyroidism of 30-40% despite the use of 131I activities of 500-550 MBq, and a 20-year risk of 60%.7-12 Cure rates and risk of post-irradiation hypothyroidism after 131I treatment vary considerably among studies, and depend on the size of the nodule, the activity applied, the use of fixed activity versus calculated activity based on dose per gram thyroid tissue, the degree of extra-nodular thyroid tissue suppression, ATD pre-treatment, and the presence of thyroid antibodies.9-11
More recent techniques for the treatment of HTNs include ultrasound (US)-guided percutaneous ethanol injection (PEI) and radiofrequency ablation (RFA). In very experienced hands, euthyroidism has been achieved in 70-90% of patients, with a less than 1% risk of posttreatment hypothyroidism during a median follow-up of 2.5-5 years,13,14 However, today most centres have abandoned the use of PEI because of its patient burden caused by the multiple treatment sessions (5 to 15 max) required to achieve euthyroidism, concern about the risk of ethanol diffusion outside the thyroid capsule causing local nerve or vascular damage, and the relatively high recurrence rate of hyperthyroidism after long-term follow- up.4,12
Treatment of HTNs by RFA has been introduced by two different groups at about the same time in 2008.15,16 Deandrea et al. used a fixed electrode position in the node’s centre, whereas Baek et al. developed the so-called moving shot technique where the electrode is moved under US guidance to produce multiple small, heat-induced ablation zones throughout the thyroid node.17 The moving shot technique has become the technique of first choice because of its higher efficacy.16 The extensive 10-year experience with moving shot RFA for non-functioning benign thyroid nodules has shown that it is capable of reducing nodal volume by 50-80%, at a very low complication rate.18,19 Global RFA experience with the aim to induce euthyroidism in patients with HTN is still limited. As of July 2019, a total of only 167 cases have been reported by centres in South Korea, China, Italy, and Austria. These studies have shown a risk of hypothyroidism of less than 3%.20-25 In the present study, we describe our experience of the first 21 patients treated in our centre. Primary aim was to establish the percentage of patients achieving a normalisation of serum free thyroxine (FT4), free triiodothyronine (FT3), and thyroid stimulating hormone (TSH) during a follow-up of one year. Nodal volume reduction and adverse effects were secondary outcome parameters.
PATIENTS AND METHODS
All consecutive patients presenting with symptomatic HTNs between May 2015 and May 2018 were included in this study. Inclusion criteria were: 1) symptoms suggestive of hyperthyroidism; 2) documented biochemical hyperthyroidism, defined as a suppression of serum TSH below the lower limit of normal (LLN: 0.3 mU/l), with FT4 or FT3 levels within or above the population normal range; 3) absence of TSH-receptor antibodies (TRab); 4) presence of a single hot nodule on 123I scintigraphy, corresponding with a well-demarcated nodule by US with a diameter of 20-50 mm; and 5) a post-RFA follow-up of at least one year. All patients meeting the inclusion criteria received verbal and written information about reported cure rates and adverse effects of RAI therapy and RFA and were free to choose either procedure. Without exception, all patients preferred treatment by RFA, mainly because they wished to avoid hypothyroidism. The study was approved by the local ethical committee (study number 2018-1335), and all patients gave their informed consent. 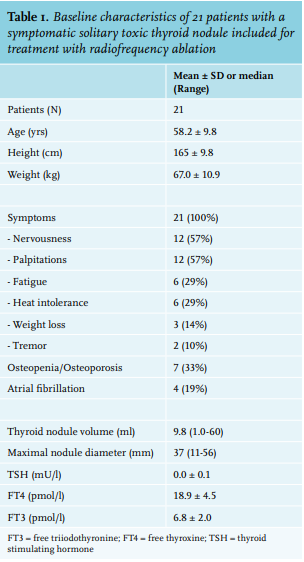
Laboratory tests
Serum TSH, FT4, and FT3 concentrations were measured on a Modular E170 (Roche Diagnostics, Almere, The Netherlands), and TSH receptor antibodies were measured on an Immulite 2000 (Siemens Healthcare, Den Haag, The Netherlands). Reference values were: TSH 0.30-4.2 mU/l; FT4 12-22 pmol/l; FT3 3.1-6.8 pmol/l; TRab < 1.0 U/l. The TSH detection limit was 0.005 mU/l.
Ultrasound
Thyroid imaging by ultrasound was performed by one of three dedicated thyroid radiologists, using a 12.5 MHz linear probe (Epic 5G, Philips Medical systems, Best, The Netherlands). Nodule dimensions and volume were assessed by measurement of three orthogonal nodule diameters (a, b, and c). The nodule volume was calculated by the equation: V = 1 /6 (πabc), where a represents the maximum diameter, and b and c, the other two perpendicular diameters. Nodule composition was assessed subjectively, and classified as solid if the solid tissue component was > 75%, and as cystic if the cystic component was > 75%. All other nodules were classified as mixed type.
123I scintigraphy
Thyroid imaging was performed with 123I in a dose of 15 MBq and assessment of 24-hour uptake with a high-energy, high-resolution collimator (Brightview XCT v2.5, Philips Medical Systems, Best, The Netherlands). Two types of images were observed: images with a single hotspot without any uptake in surrounding thyroid tissue (complete suppression), and images with a single hot spot with some uptake in the surrounding thyroid tissue (partial suppression).
RFA procedure
Platelet inhibitors were discontinued seven days before RFA, vitamin K antagonists three to five days, and DOACs 48 hours prior to treatment. RFA was performed in an outpatient day care setting, under local anaesthesia. Anxious patients received oxazepam 10 mg orally upon request, one hour before the procedure. Local anaesthesia was achieved by a US-guided lidocaine 2% injection in the skin and around the thyroid capsule. Mixed and cystic nodules were first treated by aspiration of all cyst fluid to obtain a solid nodule amenable to RFA. RFA was performed by one of three dedicated radiologists, with a Viva RF generator (STARmed Seoul, South Korea) and an 18-gauge internally-cooled electrode with a 10 mm active tip (Star RF Electrode, STARmed, Seoul, South Korea), using the trans-isthmic approach and the so-called moving shot technique, as described previously.17 The applied power ranged from 30 to 50 Watt. Voice testing and assessment of pain sensation was performed frequently during the RFA procedure to avoid any damage due to overheating of surrounding tissues. After completion of RFA, all patients remained under observation for two hours in the day care ward. Oral paracetamol 1000 mg four times daily was prescribed for one day.
Follow-up
Follow-up after RFA included measurements of FT4, FT3, and TSH at 1, 4, 13, 26, and 52 weeks, and measurement of nodule volume by ultrasound at 13, 26, and 52 weeks. Repeat 123I scintigraphy was performed at 52 weeks.
Statistics
Results are shown as mean values ± standard deviation or as median values with range. The effects of treatment over time were analysed by the Kruskal-Wallis and the Wilcoxon rank-sum tests. P values < 0.05 were considered as statistically significant.
RESULTS
A total of 21 patients were included. Their baseline characteristics are shown in table 1. All patients had at least one symptom suggestive of hyperthyroidism. Nervousness and palpitations were most common, followed by fatigue, heat intolerance, weight loss, and tremor. One-third had a diagnosis of osteopenia or osteoporosis, and one-fifth had atrial fibrillation for which they received a beta blocker and oral anticoagulation by DOAC. Ten patients had incomplete suppression of extra-nodular thyroid tissue. The majority of patients were treatment naïve; only two patients had received pre-treatment with thiamazole 5 mg daily, but this was discontinued one week before RFA. Follow-up after RFA ranged from 1.3-4.1 years, with a median of 2.5 years.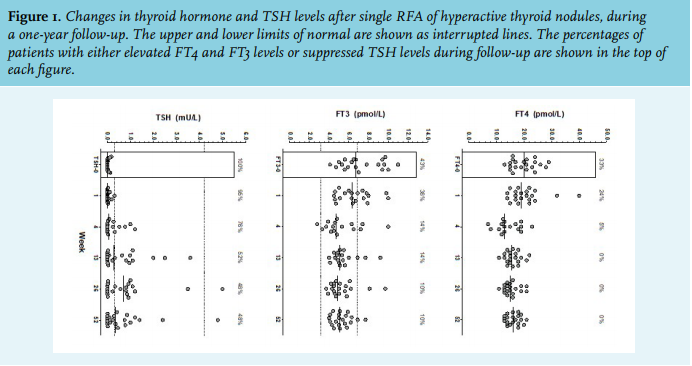
At baseline, all patients had serum TSH levels below the LLN, with TSH levels below assay detection limit in 8/21 (38%) patients. FT4 and FT3 levels were above the upper limit of normal in 33% and 43% of patients, respectively (figure 1). Maximal nodule diameters at baseline ranged from 11-56 mm (median 37 mm), with nodule volumes ranging from 1.0-60 ml and a median of 9.8 ml (figure 2). Five patients had central cystic degeneration, and 4-12 ml cyst fluid (median 5.0 ml) was aspirated to obtain a solid nodule amenable to RFA treatment. RFA was performed with a power of 30-55 Watt (median 45 Watt), applying a median of 4.4 kcal (range 1.5-10 kcal). Procedure duration ranged from 3-16 minutes with a median of 10 min. Major volume reduction was observed after three months, with stabilisation after six months. The median volume reduction at 12 months was 64% (p < 0.0001, figure 2). This decreased to 61% after correction for fluid aspiration in the five patients with central cystic degeneration. 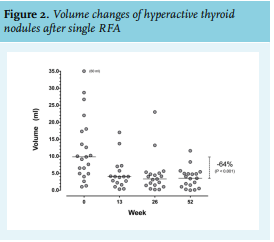
The decline in volume was directly proportional to the amount of energy applied (r = 0.74, p < 0.005). Two patients had worsening of hyperthyroidism due to RFA-induced thyroiditis, with FT4 levels rising from 24 to 40 pmol/l and from 21 to 32 pmol/l, respectively, in the first week after treatment (figure 1). This was followed by mild but persistent, antibody-negative hypothyroidism in the first patient, which required levothyroxine 50 mg daily to achieve normal TSH levels. Spontaneous recovery occurred in the second patient within four weeks. Another two patients developed transient post-thyroiditis hypothyroidism with FT4 nadir levels of 8 and 11 pmol/l, but with full recovery within four weeks. The main reduction of thyroid hormone levels was achieved after three months, with only minimal changes thereafter. At 12 months, FT4 and FT3 levels were within the normal range in 100% and 90% of patients, respectively, and TSH had increased to levels within the normal range in 11 patients (52%) without medication, and in one patient under treatment with levothyroxine 50 mg daily. The other nine patients had persistent TSH suppression. Two had become asymptomatic and did not wish additional treatment. Seven had mild but persistent symptoms of hyperthyroidism. One chose to be treated with RAI and became euthyroid after a dose of 196 MBq, and one patient preferred thiamazole 5 mg monotherapy. A second RFA was performed in five patients, and this normalised TSH levels in four out of five. This raised the post-RFA remission rate to 71%. Recurrence of hyperthyroidism was not observed during follow-up.
Repeat 123I scintigraphy was performed in 15 patients one year after RFA. At 12 months, 24-hour 123I uptake had decreased from 27 to 19%. Normalisation of uptake distribution in both thyroid lobes occurred in five patients. Hot nodule uptake remained visible in 10 patients, with unchanged suppression of the contralateral lobe in five patients and improved contralateral uptake in the remaining five patients.
Adverse effects
During the procedure, transient mild pain at the site of treatment was common, sometimes radiating to the lower jaw or ear. Pain rapidly disappeared after brief interruption of the procedure, lowering of wattage, or repositioning of the electrode. Other adverse effects were not observed. Any post-procedural pain was well controlled with paracetamol 1000 mg four times a day, and most patients stopped this medication after one day. There were no long-term adverse effects.
DISCUSSION
This study shows that RFA treatment of HTNs is a feasible option. It induced permanent euthyroidism in 52% of patients after the first RFA and this increased to 71% after a second RFA. Only one patient developed mild, but permanent subclinical hypothyroidism with a peak serum TSH of 8.0 mU/l. Clinically-meaningful adverse effects other than transient procedural pain were not observed.
Our results are in agreement with previous studies also using the trans-isthmic approach and moving shot technique. These data are summarised in table 2, and include 188 patients with a follow-up of 12-24 months.15,20-25 Although overall global experience is still limited, the data published so far indicate that euthyroidism can be achieved in about 75% of patients (range 50-91%) and at a very low risk of hypothyroidism of only 2.7%. About 30% percent of patients required more than one treatment to achieve euthyroidism and about 10% had more than two treatments. The main differences among these moving shot studies are related to the percentage of patients with overt thyrotoxicosis, presence or absence of ATD pre-treatment, mean nodule volumes at inclusion, and varying operator experience.
The efficacy of RFA appears to be primarily determined by RFA technique and nodule size. Initially, several studies were performed with a fixed needle position in the node’s centre.16,26-28 This technique is no longer used because of its limited efficacy with a median TSH normalisation rate of only 39% (range 21-54%), which is much lower than achieved with the moving shot technique.26 The impact of nodule size was evaluated in a single centre study of 29 patients with HTN. A single RFA treatment induced euthyroidism in 86% of patients with small nodules (mean volume of 5 ml, range 3-8 ml), but only induced euthyroidism in 45% of patients with large HTNs (mean volume 18 ml, range 12-29 ml).23 Whether a second RFA procedure can improve the cure rate of large nodules was not reported.
The ultimate goal of treatment is to achieve sustained normalisation of thyroid hormone levels and TSH without medication and without the need of follow-up. This implies that the definition of complete cure should not be limited to achievement of biochemical euthyroidism but should also include normalisation of 123I uptake in both thyroid lobes. In our study, only 30% of patients met these criteria. Others reported higher complete cure rates of up to 87%, and this may be related to a smaller nodule size as well as a greater operator experience. The biochemically euthyroid patients with persistent HTN remnant uptake may be at risk to develop a recurrence of hyperthyroidism. This subset of patients will require yearly follow-up, and possibly a second RFA in due time. Persistent HTN uptake with incomplete recovery of the contralateral lobe uptake has been observed in 45% of patients (range 13-86%) that have been treated worldwide (table 2). Although recurrence of hyperthyroidism has not been reported so far, it is likely to occur sometime. Structured long-term follow-up will be important to obtain the data required for evidence-based decisions about the optimal mode of treatment in specific cases. Ablation can be expected to be incomplete in nodules positioned in the vicinity of vital structures, such as the recurrence nerve and carotid artery or jugular vein, because these so-called danger areas need to be avoided. To reduce the risk of incomplete ablation and recurrence of HTN, it may be useful to include US flow measurements as standard procedure and to proceed with RFA until all nodule flow has disappeared.
The major advantage of RFA for HTNs is its very low risk of post-treatment hypothyroidism and the lack of radiation exposure. Out of 188 cases, only five (2.7%) developed hypothyroidism, and in all but one case, it was mild with TSH levels less than 10 mU/l (range 4.9-8.0 mU/l). De novo anti-TPO antibodies were detected in two of these subjects. So far, follow-up after RFA is two years or less in most cases. We therefore do not know whether the incidence of post-RFA hypothyroidism will increase on the long-term. However, this is considered to be unlikely because RFA is a local treatment, sparing extra-nodal thyroid tissue. 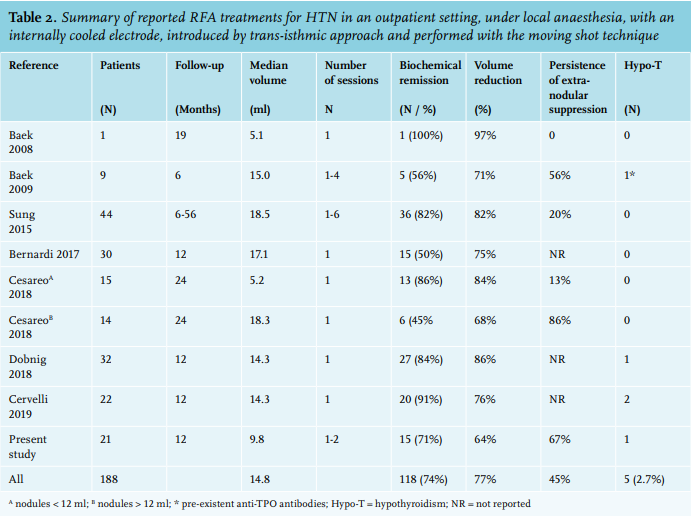
As discussed previously, normalisation of thyroid hormone levels can also be achieved with surgery or RAI treatment, however, this is associated with a relatively high risk of hypothyroidism, of up to 30% after lobectomy and to about 30-60% after RAI treatment. This implies that patients treated by surgery or RAI will require laboratory follow-up for several years, and if they develop hypothyroidism, levothyroxine treatment and biochemical monitoring will be needed for life. Prolonged follow-up is unlikely to be necessary after successful RFA, however, long-term data will be needed to prove that point. With these considerations in mind, a reappraisal of the currently available treatment modalities for HTN seems to be warranted.
In conclusion, results published on RFA so far, indicate that RFA may be considered as a candidate treatment of first choice for HTN. Euthyroidism can be expected in about 75% of patients, with a less than 3% risk of hypothyroidism. Currently available data suggest that surgery might be preferable in large HTNs and that RAI might be used as treatment in patients where surgery or RFA is contraindicated, or RFA fails to restore euthyroidism. However, the optimal indications for each of these treatments remain to be determined in future studies with long-term head-to-head comparison of RFA and RAI.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES