DIAGNOSIS
ELISA and Western blot analysis revealed seropositivity for Borrelia burgdorferi (IgM and IgG) confirming the diagnosis of Lyme carditis.
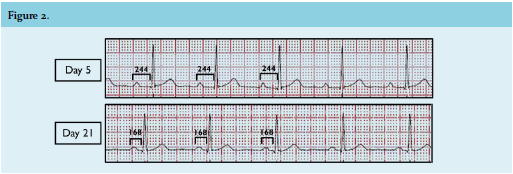
Lyme carditis represents a rare manifestation of Lyme disease, a tick-borne disease caused by Borrelia burgdorferi. Cardiac involvement in Lyme disease is estimated to occur in 0.3-4% of infected adults without appropriate antibiotic treatment in Europe.1 Atrioventricular (AV) block, being the most common presentation of Lyme carditis, can fluctuate rapidly, and progress from a prolonged PR interval to a His-Purkinje block within minutes to hours and days. It is considered that Lyme carditis occurs as a result of an inflammatory response to the presence of bacteria in cardiac tissue, most commonly in the AV node. Symptoms of Lyme carditis include syncope, shortness of breath, palpitations and chest pain, although AV block can be the sole manifestation of Lyme disease. Our patient could not recall any signs of tick bite or skin lesions representing erythema migrans. If promptly recognised, adequate treatment may completely reverse the AV block, thereby preventing fatal arrhythmias and the unnecessary implantation of a permanent pacemaker. Treatment of patients with AV block or other cardiac manifestations associated with early Lyme disease consists of oral or parenteral antibiotic therapy for 14 to 21 days. All patients with third-degree AV block should be hospitalised and continuously monitored.2,3 Our patient was immediately treated with intravenous ceftriaxone. Five days after treatment was started, the AV conduction improved from a third-degree AV block to a first-degree AV block with a PR interval of 244 milliseconds (figure 2). Once the ECG showed improvement and she became asymptomatic, intravenous antibiotics were switched to oral doxycycline, and the patient was discharged. After 21 days of treatment with antibiotics, ECG showed complete normalisation of the AV block with a normal PR interval of 168 milliseconds (figure 2).
REFERENCES