KEYWORDS
IgG4-related disease, DMARDs, azathioprine, hydroxychloroquine, mycophenolate mofetil, rituximab, methotrexate, infliximab, clinical outcomes
INTRODUCTION
IgG4-related disease (IgG4-RD) is a systemic fibro-inflammatory disease potentially affecting all parts of the human body.1 Eventually fibrosis may lead to irreversible organ damage and even secondary amyloidosis may occur.2 Therefore early recognition and swift initiation of adequate therapy remain critical.3-5
The pathogenesis of IgG4-RD is still unclear and the trigger causing the inflammation seen in IgG4-RD is unknown, but recently evolving knowledge is leading to a better understanding of the disease. The elevated IgG4 levels and the good response of IgG4-RD patients to treatment with rituximab (B-cell depletion treatment), suggest a role of the humoral immune system in the pathogenesis of IgG4-RD.6,7 IgG4 positive B-cells have been studied in IgG4-RD demonstrating increased numbers of blood IgG4 positive B-cells in patients compared to controls.8,9 In addition, oligoclonally circulating total plasmablasts are increased and appear to play a role in IgG4-RD, while the number of plasmablasts decreased after B-cell depletion.6,10,11 These plasmablasts show extensive somatic hypermutation (SHM) in the rearranged variable regions, which indicates a T-cell dependent response.11,12 Different T-cell subsets have been studied in IgG4-RD and have shown that T-cells are also important in the pathogenesis of IgG4-RD.6,9,13 T follicular helper 2 (Tfh2) cells are possibly involved in driving the class switch to IgG4.14 Different cytokines, including interleukin (IL)-4 derived from T-helper 2 (Th2) cells may also contribute to the pathophysiology of IgG4-RD.9,15-17 but the role of Th2 cells in IgG4-RD remains unclear.18,19 Recently, CD4+ T-cells displaying cytotoxic features appeared to be abundantly present in peripheral blood and diseased tissue sites of patients with IgG4-RD and possibly also contribute to the pathogenesis of the disease.13,20
Glucocorticoids are the first choice for treatment. The relapse rate after tapering glucocorticoids is high, hence steroid-sparing maintenance therapy is often required.21 Several disease modifying anti-rheumatic drugs (DMARDs) such as methotrexate and azathioprine have been used as steroid-sparing treatment of IgG4-RD, but studies confirming their efficacy are lacking.22 Most of the reports on the use of steroid-sparing treatment with DMARDs are case-based reports.23 Emerging data from case series reveal promising results for rituximab in the treatment of patients with IgG4-RD.1,24-26 The aim of the current study is to evaluate the different treatment outcomes in a well-defined cohort of patients with IgG4-RD.
MATERIALS AND METHODS
The Erasmus University Medical Center is a tertiary referral centre for patients with IgG4-RD. All patients diagnosed with IgG4-RD are treated and monitored prospectively. However, patients may also be diagnosed with IgG4-RD retrospectively. Medical records of patients with IgG4-RD between 1999 and April 2017 were reviewed for demographic and clinical characteristics. Only patients with histologically confirmed IgG4-RD according to established Boston criteria for histology were included.27 The efficacy of all therapies including glucocorticoids, DMARDs (mycophenolate mofetil, methotrexate and azathioprine), hydroxychloroquine, cyclophosphamide, rituximab, thalidomide, infliximab, surgery and radiotherapy were evaluated. The disease activity in patients was evaluated using the IgG4-related disease Responder Index (IgG4-RD RI), a monitoring tool for disease activity in IgG4-RD using the clinical, laboratory and radiological outcomes. IgG4-RD RI is designed for the physicians to easily score the extent of the disease activity. A score of 0 signifies the absence of active disease in an organ, a score of 1 indicates improvement of the disease activity within an organ, a score of 2 indicates that the disease within an organ has remained unchanged, a score of 3 indicated the presence of new or recurrent disease activity and a score of 4 refers to disease that has worsened despite treatment. The levels of serum IgG4 are scored as same manner and scored according to normal, improved, persistent or new/recurrent/worsened despite treatment.28
Active disease was defined by an IgG4-RD RI score of ≥ 3.29,30 Improvement in the disease activity and complete response are defined as a decline of ≥ 2 points compared to the baseline score or IgG4-RD RI of < 3 and decline ≥ 2 after treatment, respectively. Partial response and disease relapse were defined as a decline of ≥ 2 points in IgG4-RD RI, but still ≥ 3 and worsening of clinical, radiological and serological (serum IgG4) findings, respectively. This study was performed according to the Declaration of Helsinki and was approved by the Medical Ethics Committee of Erasmus MC (ethics approval numbers MEC-2017-1169).
RESULTS
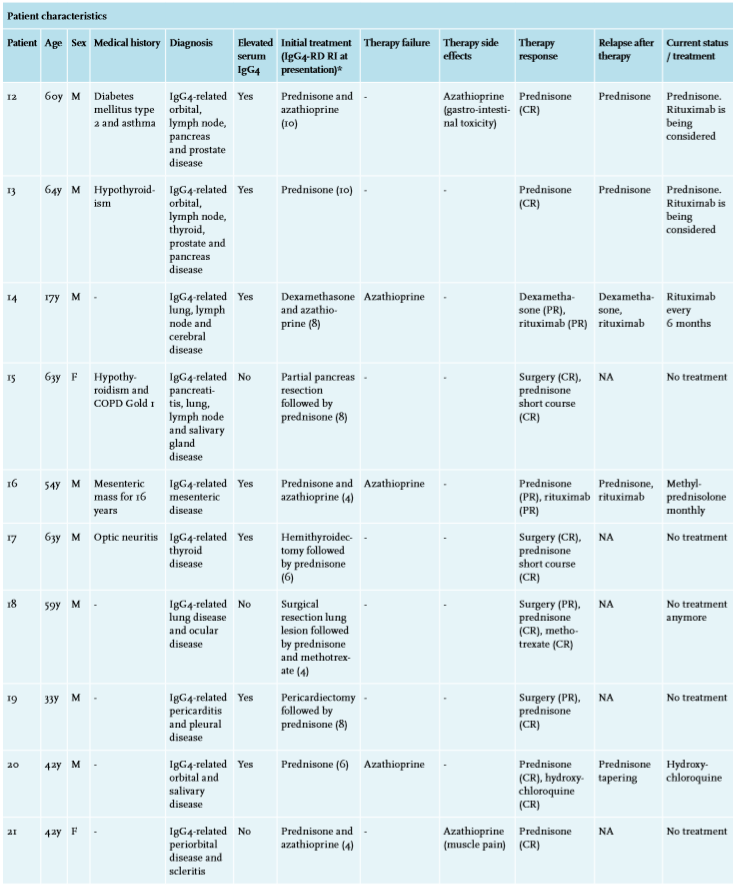
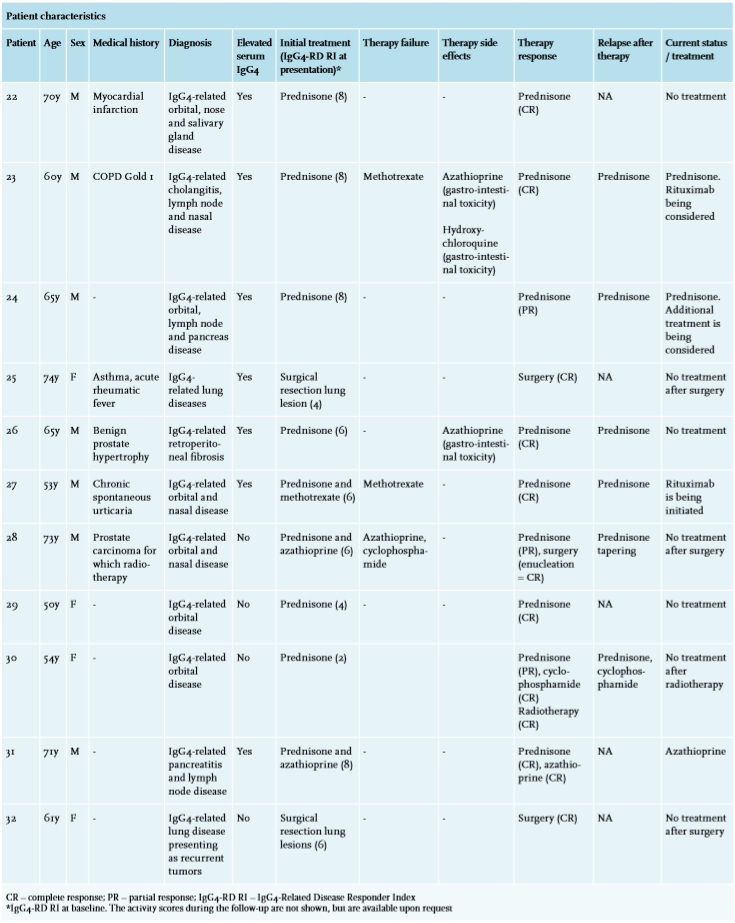
All together 32 patients with IgG4-related disease were included with a mean age of 57 years, ranging from 17 to 77 years, of which 72% were male. The main outcomes of this study are presented in table 1. An overview of the different treatment modalities in these 32 patients is presented in table 2A and the different treatment outcomes (response, failure and relapse) for each treatment strategy are demonstrated in table 2B. The patients represented a heterogeneous group of IgG4-RD with different organ manifestations. Most of the patients had ocular (53%) manifestation of the disease. The medical history was unremarkable in most of the cases, though five patients had asthma. All the cases were histologically confirmed using the Boston consensus criteria for histology.27 Almost all patients (29/32 = 91%) were treated with glucocorticoids (mostly prednisone 0.5-1 mg/kg/day) leading to clinical response in all. In the remaining three patients, initial treatment with methotrexate followed by hydroxychloroquine in one patient and surgery in two patients led to complete response. In 27 (out of 29) patients glucocorticoids were started initially and in two after relapse or failure of the initial glucocorticoid sparing regime (patients 4 and 6). In 10 (out of 27) patients glucocorticoids were initiated as monotherapy; in the remaining patients these were combined (table 2A). Complete response was observed in 72% of the patients receiving glucocorticoids, whereas 28% showed a partial response. Glucocorticoids were usually continued for a period of four to six weeks and thereafter tapered slowly and withdrawn in a period of three months up to one year. In just two patients a short course of prednisone was started after initial surgical excision of the affected tissue. Despite a good initial clinical response a flare of the disease occurred when the glucocorticoids were tapered or discontinued in 62% of the patients, necessitating additional (steroid-sparing) treatment. 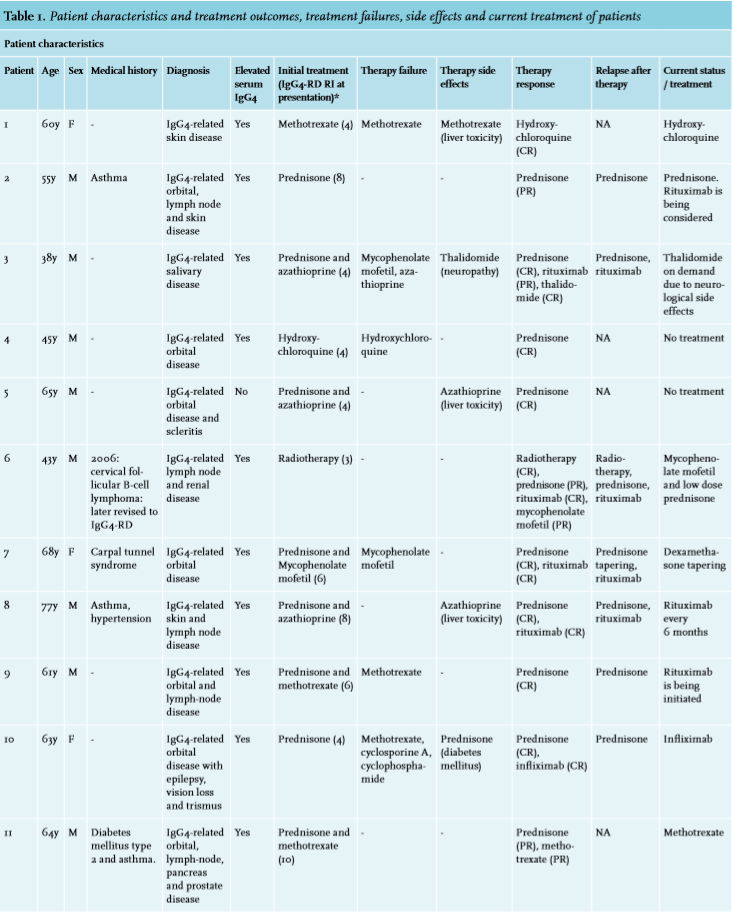
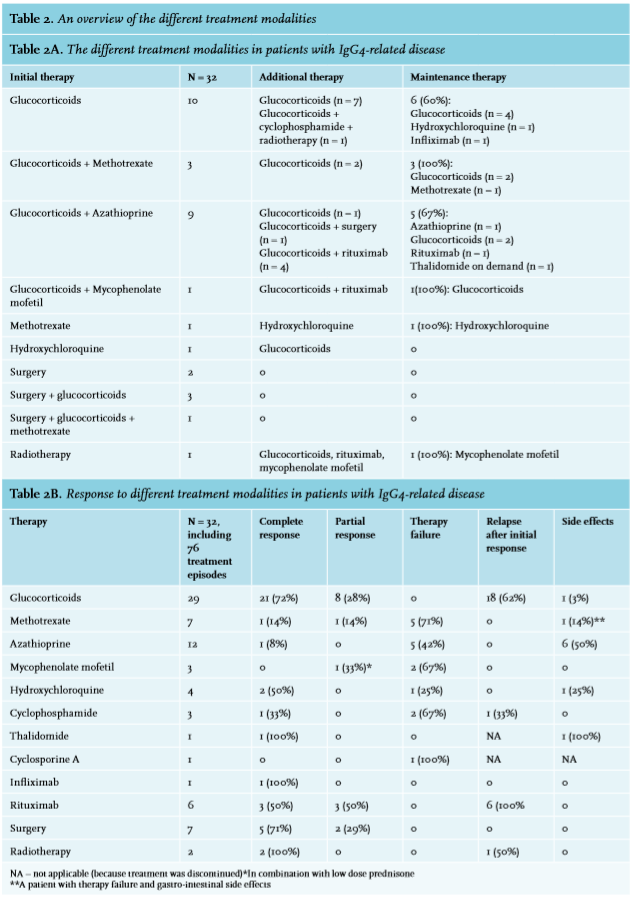
Methotrexate was initiated in seven patients, usually in a dose of 15 mg per week, which proved effective in a minority of two (29%, one complete response and one partial response). In the five other patients methotrexate failed to suppress the disease activity, in one case also causing gastro-intestinal toxicity.
A total of 12 patients were treated with azathioprine, with only one complete response (8%), a patient with pancreas and lymph node involvement in which azathioprine was successfully continued as maintenance treatment after prednisone induction therapy. In six out of 12 patients (50%) azathioprine was terminated because of toxicity (liver, gastro-intestinal, muscle symptoms) before disease activity could be assessed. In the remaining five patients azathioprine proved insufficient to suppress the disease activity and led to discontinuation of this treatment (treatment duration > 3 months).
Mycophenolate mofetil was initiated as maintenance treatment after steroid induction in three patients. Two patients showed treatment failure. One patient, with renal and lymph-node involvement of IgG4-RD refractory to prednisone tapering, azathioprine and rituximab showed a partial response with low dose prednisone and mycophenolate mofetil.
In four patients hydroxychloroquine was used as a maintenance therapy, showing complete response in two (50%), after initial therapy with methotrexate and prednisone respectively. In one (25%) patient initial therapy with hydroxychloroquine was ineffective and replaced by prednisone resulting in clinical remission. In another patient hydroxychloroquine was withdrawn because of gastro-intestinal side effects.
Cyclophosphamide was used in 3 patients with organ function threatening disease after induction treatment with prednisone, which caused complete remission of the disease in one patient (33%), albeit only temporary.
As regards other agents, cyclosporine A was used once without clinical effect. Thalidomide was initiated in one case of therapy refractory salivary disease leading to complete remission of the disease. However, the patient experienced neurological side effects and is using thalidomide now on demand.
Infliximab was used once in a patient with orbital disease refractory to prednisone tapering, methotrexate, cyclosporine A and cyclophosphamide. Infliximab has induced a complete remission and the disease has been in remission for more than five years.31
Rituximab was initiated, usually as a third line treatment, in six patients by way of maintenance therapy (50% complete response, 50% partial response). Hoever, the clinical remission after a single dose of 2 grams observed in these patients was temporar. All patients relapsed within six months to two years after initiating rituximab. Two patients who relapsed after treatment with rituximab are currently receiving rituximab every six months with complete remission of the disease.
Primary surgical intervention in seven patients, including hemithyroidectomy, resection of pulmonal masses, pericardiectomy and partial pancreas resection, led to durable complete responses (median = 36 months). In two cases with solitary pulmonary involvement, resection of the lung lesions was performed and there was no further indication for systemic immunosuppressive therapy. In one case with orbital and nasal involvement, enucleation of the eye was eventually performed because of persistent symptoms of pain after treatment failure with regard to prednisone tapering, azathioprine and cyclophosphamide. The enucleation led to clinical remission and pain symptoms resolved. Diagnosis of IgG4-RD was established retrospectively after enucleation.32 In two other patients a short course of prednisone after surgery was sufficient to achieve complete remission of the disease. Furthermore, radiotherapy was used in two patients for lymph node involvement and therapy refractory IgG4-related orbital disease respectively, causing complete remission in both cases. The patient with lymphadenopathy developed a recurrence of the lymphadenopathy with new onset renal involvement of the disease a couple of years later, for which the patient started on systemic immunosuppressive therapy. The other patient is in clinical remission five years after radiotherapy.
DISCUSSION
In this study we describe the treatment outcomes in 32 IgG4-RD patients with various organ manifestations. The observations clearly indicate that the treatment of IgG4-RD can be challenging and must be patient specific. The current study represents a heterogeneous cohort of patients with various organ manifestations. As in most studies, IgG4-RD patients were middle-aged and mostly men.21 However, in a previously published systemic review we demonstrate that IgG4-RD can also affect children of all ages.33
Glucocorticoids
Glucocorticoids are commonly initiated as immunosuppressive induction therapy. Various types of cells of the immune system, including B and T-cells and macrophages, can be affected by glucocorticoids.34 Glucocorticoids are considered the mainstay treatment of IgG4-RD and usually effective in a dose of 0.5-1.0 mg/kg/day, depending on severity or organ threatening character of the disease despite the absence of randomized clinical trials.1,22,35 In the current study a high response rate is followed by swift recurrences after tapering prednisone at levels corresponding to previous reports.22 The high response rates warrant the use of glucocorticoids as first line treatment despite the frequent recurrences. Such high recurrence rates emphasize the need of alternative steroid-sparing therapy, which has been advocated in many case series.22 The results in the current study of alternative treatments are discussed below.
Azathioprine
Azathioprine is frequently used in immune mediated diseases.36 Among DMARDs, the use of azathioprine has been most frequently reported in patients with IgG4-RD, especially in IgG4-related pancreatitis.29 According to the consensus guidance, azathioprine, methotrexate or mycophenolate mofetil may be initiated as prednisone sparing therapy in IgG4-RD.22 A recent study of 18 patients showed therapeutic efficacy for azathioprine in preventing relapse with IgG4-related pancreatitis.37 Furthermore, case reports have suggested azathioprine to be effective in several manifestations such as IgG4-related cholangitis, IgG4-related kidney disease and hypophysitis.38-40 In the presented study however, azathioprine appeared effective in only a minority of cases (8%). The only patient with a clinical response to azathioprine had inflammatory pancreatic disease and enlarged lymph nodes. The remaining 11 patients had disease manifestations without pancreatic involvement. Therefore azathioprine may serve as second line therapy for the subgroup of patients with pancreatic localizations. Remarkably, the continuation of azathioprine was restricted because of toxicity in a substantial number of patients. This toxicity is unfamiliar at such high percentages. It remains of interest whether this is a disease specific complication. Therefore the efficacy of azathioprine in IgG4-RD remains unclear.
Methotrexate
Except for two small studies suggesting methotrexate as a good steroid-sparing drug,29,41 its application in IgG4-RD has only been described in limited case reports.42 Methotrexate affects the function of memory T-cells that produce pro-inflammatory and pro-fibrotic cytokines and is therefore a drug of interest in the treatment of IgG4-RD.43 In the current study however, methotrexate does not seem to be particularly beneficial, despite its low toxicity.
Mycophenolate mofetil
Mycophenolate mofetil selectively inhibits cytotoxic T-lymphocytes and is being used as an anti-inflammatory agent. Furthermore, mycophenolate mofetil is related with anti-fibrotic effects possibly due to inhibition of the transforming growth factor beta pathway44 and can therefore be a potentially interesting drug in the treatment of IgG4-RD. Just like the other DMARDs, mycophenolate mofetil has not been studied in large cohorts, but has been reported in case reports.45-48 In the current study, mycophenolate mofetil caused partial remission in combination with low-dose prednisone in only one of three patients without toxicity. The use of mycophenolate mofetil therefore may be evaluated in larger cohorts.
Hydroxychloroquine
Hydroxychloroquine was initially designed as an antimalarial drug, but because of the accompanying antirheumatic effects it has become widely used in rheumatic and autoimmune disease. The exact role of hydroxychloroquine has not been identified, but it is believed that it has anti-inflammatory and possibly also anti-fibrotic effects.49-51 In the current study hydroxychloroquine was initiated because of its positive outcomes in other inflammatory diseases like sarcoidosis.52 There are no published reports on hydroxychloroquine in IgG4-RD, but it is often used in the treatment of other immune mediated diseases. In our study, hydroxychloroquine was used in four cases as maintenance therapy and showed complete response in two patients (50%). Gastro-intestinal complaints led to withdrawal of hydroxychloroquine in one patient (25%). Generally, the drug is not associated with severe adverse effects except for retinal toxicity at higher doses.53 The efficacy of hydroxychloroquine needs to be evaluated in larger cohorts, but in cases of less severe IgG4-RD it may be useful.
Cyclophosphamide
Cyclophosphamide has been regarded ineffective in IgG4-RD.54 However, in a recent study cyclophosphamide yielded a lower relapse rate when combined with glucocorticoids relative to monotherapy with glucocorticoids.30 In the present study three patients with organ threatening disease were treated with cyclophosphamide and glucocorticoids, because of relapse or failure to respond to DMARDs. Patients treated with cyclophosphamide were those diagnosed with IgG4-RD retrospectively. Only one patient achieved a temporarily complete remission. Use of cyclophosphamide in IgG4-RD should therefore be restricted to cases where no other therapy is available in organ threatening disease.
Rituximab
The B-cell ablative chimeric monoclonal antibody rituximab is an emergent effective treatment strategy for IgG4-RD.1 however, large randomized controlled studies have not yet been performed. Despite the good clinical response, the relapse rate after treatment with rituximab is high.26 In the current study, clinical remission occurred in all six patients treated with rituximab (50% complete response versus 50% partial response). Rituximab was initiated after failure with DMARDs or relapse after prednisone tapering. However, after single dose treatment with rituximab, the disease recurred in all patients six months to two years after initiating the treatment. One of the patients with severe IgG4-related skin disease is currently treated with rituximab 1000 mg every six months. Another patient with systemic disease and recurrence after rituximab is also being treated with rituximab every six months, a treatment strategy already used in other diseases such as granulomatosis with polyangiitis.55 As suggested previously,2 rituximab maintenance treatment is a potentially effective strategy in patients with relapses. This needs to be investigated in future studies.
Other therapeutic modalities
Cyclosporine A is a calcineurin inhibitor in which a decrease in interleukin-2 production and, therefore, T-cell proliferation is established. Carbajal et al report on a case of IgG4 related disease with cardiac involvement which was refractory on mycophenolate mofetil, azathioprine, methotrexate, or cyclophosphamide, but in the end could be treated with prednisone in combination with cyclosporine.56 Cyclosporine A was used once in our study without any clinical effect.
Thalidomide has previously been shown to be effective in two patients with IgG4-related skin disease.57 Because of therapy refractory salivary disease due to IgG4-RD, one patient in our study was successfully treated with thalidomide. Its mechanism of action is not completely understood but suppression of TNF-α production is considered a possibility.58 However, neurological side effects of thalidomide may lead to discontinuation of this treatment. Infliximab, a chimeric monoclonal antibody against TNF-α, has only been reported in one case report. In our study, one patient was successfully treated with infliximab after treatment failure with methotrexate, cyclosporine A and cyclophosphamide.59 Fibrosis, a hallmark of IgG4-RD, has been associated with overexpression of TNF-α and might be a target for infliximab and thalidomide.59
Surgery
IgG4-RD mostly presents as tumor-like infiltrations and can therefore be treated by surgery in certain cases.21 Surgical treatment of IgG4-RD often leads to regression of the disease.60-62 Patients primarily treated with surgical intervention in our study proved recurrence free after long-term follow-up. Numbers are small, but they suggest a favorable outcome, so surgical incision/resection of the disease should be considered.
Radiotherapy
Radiotherapy has been reported successful in IgG4-RD,63,64 in the current study causing complete remission in one patient with therapy refractory orbital disease and another patient with IgG4-related lymphadenopathy. After a couple of years the patient with lymphadenopathy developed a recurrence, but the patient with orbital disease has been in remission for five years now. In this case, the disease was previously refractory to prednisone and cyclophosphamide but eventually responded very well to radiotherapy. Radiotherapy can be considered as a possible treatment strategy for localized and symptomatic therapy in refractory IgG4-RD.
CONCLUSION
In this observational study of 32 patients with IgG4-RD, we demonstrated the different treatment outcomes. The rarity of the disease and its many different manifestations at the time of diagnosis make assessing the optimal treatment into a challenge. This study has some limitations. First of all, all the data are observational. The choice of treatment was based on recommendations in the existing literature and the experience of the prescribing immunologist. Furthermore, patients in this cohort presented with IgG4-RD with different organs involved. The treatment outcome could be different, based on the type of organ involved. Unfortunately the cohort described in this study is too small to perform any sub-analyses. Ideally the choice of treatment would be investigated in a randomized controlled trial. This is a challenge on account of the rarity of the disease.
Nevertheless, this study shows that glucocorticoids and rituximab induce substantial responses, as do primary surgical intervention and radiotherapy. The efficacy of DMARDs is limited. Alternative strategies with hydroxychloroquine, thalidomide and infliximab look promising. More data are needed to confirm these observations, so as to arrive eventually at evidence based treatment guidelines, improving the treatment of patients with IgG4-RD disease.
RECOMMENDATIONS
The treatment of IgG4-RD is often challenging. Previously small reports have emphasized the efficacy of DMARDs in IgG4-RD, which unfortunately we did not observe. The current consensus guidance however recommends treatment with DMARDs as a second line treatment option in IgG4-RD patients. Larger prospective studies are required to understand the role of DMARDs in IgG4-RD. Based on current knowledge we recommend the following treatment strategy in IgG4-RD:
Use the IgG4-RD RI to establish the disease activity and to monitor the disease activity
Check whether there is a treatment indication taking into account that IgG4-RD almost always requires treatment because of the likelyhood of secondary complications;
Whenever possible, for example in a patient with single organ manifestation of the disease, surgery is preferred because of the favourable disease course with possibly fewer relapses. Consider a short course of glucocorticoids after surgery;
Glucocorticoids (usually prednisone 0.5-1.0 mg/kg/day or equivalent) are preferred as first line therapy for IgG4-RD. The initial dosage of glucocorticoids should be maintained for two to four weeks. Thereafter, glucocorticoids can be tapered slowly. It is recommended to continue using glucocorticoids for three to six months;
In case of relapse after tapering glucocorticoids, consider DMARDs as a second line treatment. In case of severe disease activity, consider rituximab as second line treatment;
In case of liver and pancreas manifestation of the disease, azathioprine should be considered. In case of other organ manifestations, consider methotrexate, mycophenolate mofetil or hydroxychloroquine if the (vital) organs are not threatened. The patients should be monitored frequently in order to keep tabs on the disease activity and avoid possible side effects of the DMARDs;
Consider radiotherapy if organs are threatened by the mass effect of tumor/IgG4-RD;
Rituximab should be started as a third line treatment of IgG4-RD, or earlier in the treatment course when vital organs are affected. Consider rituximab maintenance therapy after induction of 2 grams of rituximab. Evaluate after a couple of years of treatment whether the maintenance therapy can be discontinued;
Further treatment options include cyclophosphamide, to be considered in therapy refractory cases. Rituximab is clearly preferred over cyclophosphamide. Also In patients with therapy failure thalidomide may be considered.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES