KEYWORDS
Infant adequate intake; iodine; iodine status; lactation; pregnancy
INTRODUCTION
Iodine is necessary for the formation of thyroid hormone.1 Iodine deficiency can cause hypothyroidism. During pregnancy this may lead to pregnancy complications and impaired brain and cognitive development. Iodine is also important for infant brain development during lactation. Iodine deficiency during pregnancy occurs in West European countries, including the United Kingdom, Sweden, Denmark and Belgium.2 In the Netherlands, salt has been fortified with iodine since the Second World War. Iodised salt in bread became an important iodine source; other important sources are iodised table salt, seaweed, fish, dairy products and meat.3 Pregnant and lactating women are vulnerable to iodine deficiency. The Health Council of the Netherlands currently uses the dietary standards of the Nordic Council.4 Based on iodine requirements to prevent goitre and maintain normal thyroid function, the recommended daily intake for adults is 150 µg/day and the average requirement is 100 µg/day.5 To cover foetal needs and maintain thyroid gland function, an extra 25 µg/day is required during pregnancy. An extra 50 µg/day is recommended during lactation to provide sufficient iodine in the breast milk.5 These recommendations for pregnant and lactating women are in agreement with the European Food and Safety Authorisation (EFSA),6 but are lower than the recommendations of the Institute of Medicine (IOM).7 Iodine status is established by measurement of the urinary iodine concentration (UIC). A 100 µg/l cut-off value is employed for the general population, lactating women included. For pregnant women, the cut-off is set at 150 µg/l.8 It should be noted that these cut-offs apply for populations, not individuals. The UIC cut-offs as set by the World Health Organisation (WHO) are widely accepted, but there are nevertheless some concerns. These cut-offs are based on an average 24-hour urine volume of 1.5 litres.9 The Doetinchem study found an average of 2.0 litres in a Dutch population, suggesting an underestimation of iodine status by UIC measurement. The National Institute for Public Health and the Environment (RIVM) in the Netherlands found that, in 2007-2010, the Dutch population aged between 7-69 years ‘generally consumed sufficient amounts of iodine’. It was estimated that roughly 10% of pregnant and 50% of lactating women had iodine intakes below the estimated average requirement.10 In 2008, the maximally permitted iodine content of bakery salt in the Netherlands was reduced from 70-85 to 50-65 mg/kg salt. It was simultaneously allowed to add iodised salt to almost all foods.11 Since then iodine intake has decreased by 20-25%.12 A study in Doetinchem (the Netherlands) concluded that from 2006 to 2015, iodine intakes had declined by 37% in men and 33% in women.13 Until 2008 the iodine status of pregnant Dutch women was not a reason for concern. The Generations R Study, conducted in Rotterdam in 2002-2006, found a median UIC of 230 µg/l (90% range: 55-733 µg/l) at 13 gestational weeks (GW).14 In 2015, Dutch women of a reproductive age (19-49 years) in Doetinchem had a median (P25-P75) UIC of 76 (45-131) µg/l. Since the urine volume of the study population was higher compared with the WHO study, they might have underestimated the real iodine intake.13 The 24-hour iodine excretion and estimated iodine intake in the Doetinchem study population were [median (P25-P75)]: 139 (109-190) and 151 (119-207) µg/day, respectively. There are no data on the iodine status of Dutch pregnant women as established after the reduction of iodine in salt in 2008.
We determined the iodine status of a small group of pregnant women at 20 gestational weeks (GW). The study was a secondary aim of our ZOOG-MUM trial. In this trial we provided a multivitamin supplement containing 150 µg iodine/day. We investigated whether this dose is sufficient to reach or maintain an adequate iodine status during pregnancy and lactation. We also investigated whether the breast milk iodine concentrations (BMIC) were in line with the adequate intake (AI) for newborns.
MATERIALS AND METHODS
This was a randomised trial primarily designed to study the dose responses of supplemental fish oil and vitamin D during pregnancy and lactation. It has been named ‘ZOOG MUM’ and was conducted in Groningen, the Netherlands. A secondary aim was to study iodine status before and after iodine supplementation in an open label observational design. The participants were aware of the composition and the doses of the nutrients in the multivitamin supplement (see below under Supplements). The study was approved by the Ethics Committee of the University Medical Center Groningen (UMCG) (METc number 2014.263) and was registered in the Netherlands National Trial Register (Trial ID NTR4959). All women provided written informed consent. The study was in agreement with the Helsinki Declaration of 1975, as revised in 2013.
Study population
From December 2014 until December 2015, pregnant women in their first trimester were invited to participate. Forty-three apparently healthy women with singleton pregnancies were included. Exclusion criteria were as follows: vegetarian/vegan diet, hyperemesis gravidarum, pregnancy complications or preterm delivery and not having the intention to exclusively breastfeed after delivery. None of the participants used iodine-containing medication at the start or during the study, but most (61%) took iodine supplements prior to the beginning of the study.
Supplements
From 20 GW until 4 weeks postpartum, all participants received a multivitamin supplement (Omega Pharma; Rotterdam, the Netherlands) providing a daily dose of 150 µg iodine and 12-135% of the Dutch Recommended Dietary Allowance RDA/AI for vitamins and minerals for pregnant and lactating women. We did not verify the iodine content of the supplements. Consistent with the primary aim, they received ascending dosages of DHA-rich fish oil (315-1260 mg DHA+EPA) and vitamin D (10-85 µg/day) (both from Bonusan; Numansdorp, the Netherlands). All mothers reported adherence to the supplement protocol. They took > 75% of the supplements, as established by inquiry at appointments, by questionnaire, or both.
Sample collection
The study was started at 20 GW. The participants collected a 24-hour urine sample at the start of the study, at 36 GW and 4 weeks postpartum. At 4 weeks postpartum they also collected a breast milk sample. Urine and breast milk samples were collected on the same day. Participants were instructed to collect their urine for 24 hours, starting after emptying their bladder for the first time in the morning, until at the same time the following day when they again empty their bladder. Participants were asked to store the urine sample in a cold place and to take it along at the next appointment in the UMCG, preferably on the same day. Participants were instructed to document the time they started and ended the collection. This information was reviewed during the appointment. Completeness of the 24-hour urine collection was established by interview. To ensure that all mothers collected the milk in a similar manner, milk from a completely emptied breast was collected around noon (10.00-14.00). The milk was collected manually or by breast milk pump. The samples were homogenised by careful mixing. They subsequently divided the sample among two sampling tubes. The milk samples were stored in the participant’s freezer and taken along to the appointment in the UMCG. The 24-hour urine samples were immediately homogenised and divided into two portions. Urine and breast milk samples were stored at -20 °C until analysis.
Analysis
Iodine in 24-hour urine samples was analysed in the UMCG by inductively coupled plasma-mass spectrometry (ICP-MS; Varian, USA). The intra- and inter-assay coefficients of variation (CVs) were 1.9 and 5.9% at 40 µg/l and 0.9 and 0.5 % at 225 µg/l. BMIC was analysed in the European Laboratory of Nutrients (ELN; Bunnik) by ICP-MS (Agilent, USA). The intra- and inter-assay CVs were 6.3 and 5.5% at 0.7 µmol/l and 5.6 and 5.8% at 2.0 µmol/l.
Cut-off values for iodine insufficiency and newborn adequate intakes
The WHO has issued cut-off values for the evaluation of iodine status based on the UIC.8 The iodine status in a population is considered sufficient if the median UIC is above the cut-off value. For the general population, including lactating women, cut-off values are set at 100 µg/l. For pregnant women the cut-off value amounts to 150 µg/l.8 The WHO considers spot urine samples sufficient as day-to-day and within-day variations are averaged in a population.15 These cut-offs are, however, based on an average 24-hour urine volume of 1.5 litres.9 As we were dealing with only a small group of pregnant women, we chose to collect 24-hour urine samples and also calculated the 24-hour iodine excretion.
The Health Council of the Netherlands and the European Food and Safety Authority (EFSA) has not established an adequate intake (AI) for infants aged 0-6 months. The iodine-AI established by the IOM,7 and the Nordic Council5 are 110 (IOM-AI) and 50 (Nordic-AI) µg/day, respectively. The IOM-AI is based on average milk iodine concentrations in a group of healthy lactating women. The Nordic-AI is based on goitre prevalence and urinary iodine excretion in European children and extrapolated from adults based on energy and growth requirements. Using an average daily milk intake of 780 ml16 and 126.9 g/mol iodine atomic weight, these AIs translate to milk iodine cut-offs of 1.1 µmol/l (IOM-AI) and 0.5 µmol/l (Nordic-AI), respectively. Since these are adequate intakes, only qualitative comparison is possible. Levels below the AI merely provide indications for a higher risk of iodine deficiency that requires further research.17
Data analysis and statistics
We used IBM PASW Statistics 23 software and R studio 1.0.143. Median (ranges) were reported. Between-group differences were analysed with the Mann-Whitney U test for continuous data. Differences between data at the various time points were analysed by the Wilcoxon signed-rank test. A p value < 0.05 was considered significant.
RESULTS
Study population
Forty-three women were included. Seven discontinued the study, of whom three voluntarily and four because of pregnancy complications. At 4 weeks postpartum, three women had discontinued breastfeeding. One woman provided us with a milk sample but did not provide a 24-hour urine sample at 4 weeks postpartum. Table 1 shows the basic characteristics of the 36 women and their infants who were finally studied. 
Iodine status during pregnancy and lactation
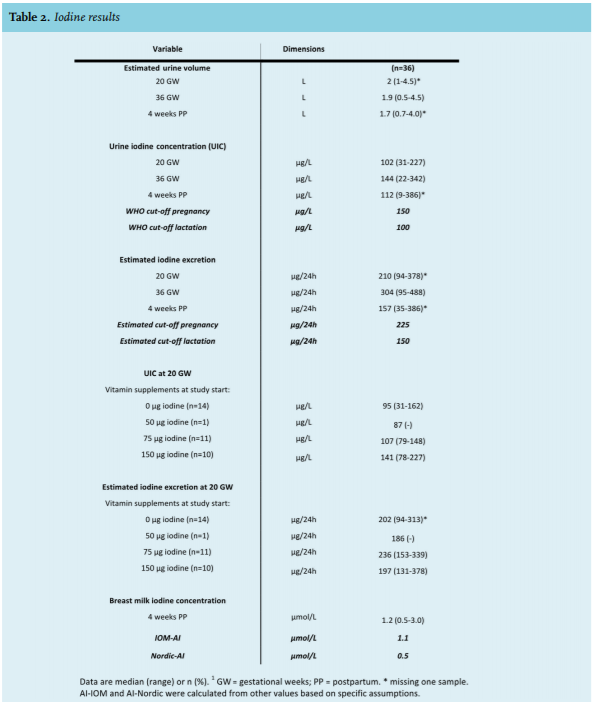
The median (range) UIC at 20 GW was 102 (31-227) µg/l (figure 1A; table 2). Median 24-hour urine volume and iodine excretion were 2.0 (1-4.5) l/24h and 210 (94-378) µg/24h, respectively. A total of 83% (30/36) had a UIC below 150 µg/l. The UIC of women who, by their own choice, took iodine-containing multivitamin supplements prior to 20 GW (61% of the women) did not differ from the UIC of counterparts who did not. However, although not significant, there was a trend in the dose response: the median (range) UICs (in µg/l) were: 95 (31-162; n = 14; for those taking 0 µg iodine/day), 87 (n = 1; 50 µg iodine/ day), 107 (79-148; n = 11; 75 µg iodine/day) and 141 (78-227; n = 10; 150 µg iodine/day) (table 2). The women ingesting the highest doses seemed to have the highest UIC.
At 36 GW the median (range) UIC had increased to 144 (22-342) µg/l (figure 1A; p < 0.01; and table 2). Median 24-hour urine volume and iodine excretion were 1.9 (0.5-4.5) litres and 304 (95-488) µg/24h, respectively. Of the women, 56% (20/36) had a UIC below 150 µg/l. At 4 weeks postpartum the UIC had decreased to 112 (9-386) µg/l (figure 1A; p < 0.01; table 2). Median 24-hour urine volume and iodine excretion were 1.7 (0.7-4.0) litres and 157 (35-386) µg/24h, respectively; 40% (14/35) had a UIC below 100 µg/l.
We found a correlation between iodine status at 20 GW and 36 GW (r = 0.459; p < 0.01), and a correlation between iodine status at 36 GW and 4 weeks postpartum (r = 0.622; p < 0.01).
Iodine in milk
Milk samples were available from 33 women. The median (range) BMIC was 1.2 µmol/l (0.5-3.0 µmol/l; figure 1B; table 2). Of the infants, 33% (11/33) had estimated intakes below the IOM-AI, while none had estimated intakes below the Nordic-AI. We did not find a correlation between UIC at 4 weeks postpartum and BMIC (r = -0.21; p = 0.905).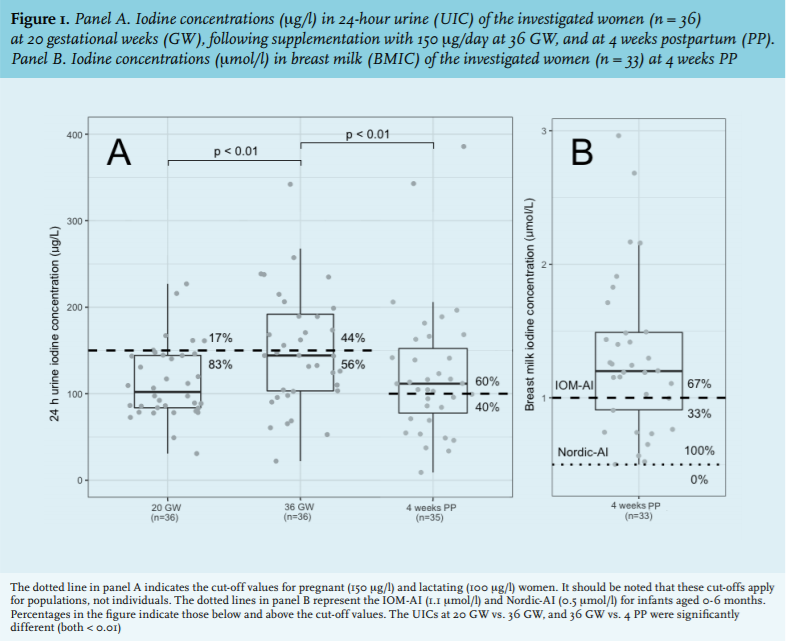
DISCUSSION
In the present pilot study, 83% of the pregnant women had a UIC < 150 µg/l at 20 GW. The median iodine excretion was 210 µg/24h. After a daily intake of 150 µg iodine the median UIC increased from 102 µg/l at 20 GW to 144 µg/l at 36 GW. The percentage women with a UIC < 150 µg/l decreased to 56% and the median iodine excretion was 304 µg/24h. At 4 weeks postpartum the median UIC had decreased to 112 µg/l, and 40% of the lactating women had a UIC < 100 µg/l. The corresponding median iodine excretion was 157 µg/24h and the median BMIC was 1.2 µmol/l. Of the infants, 33% had an estimated iodine intake below the IOM-AI, whereas none had an estimated intake below the Nordic-AI.
The median UIC of 102 µg/l at 20 GW is lower than the 230 µg/l found in 1525 pregnant women in Rotterdam in 2002-2006,14 but higher than the median UIC of 76 µg/l, as found in Doetinchem in 2015, in 98 non-pregnant women aged 19-49 years.13 A
lthough most studies collected spot urines, as opposed to the 24-hour urines in the present study, and information on 24-hour urine volumes is consequently lacking, similarly low median UICs of 87, 88, 98, 101-114, and 124 µg/l were found in pregnant women in Belgium,18 United Kingdom,19 Sweden,20 Denmark,21 and Austria,22 respectively. The current 83% of women with UICs below 150 µg/l is much higher than the 10% estimate of the RIVM for pregnant women with iodine intakes below the RDA in 2007-2010.10
The UIC cut-offs as set by the WHO are widely accepted, but there are nevertheless some concerns. First, these cut-offs are based on an average 24-hour urine volume of 1.5 litres.9 In our study we found median urine volumes of 2.0 and 1.9 l/24h at 20 GW and 36 GW, respectively, and 1.7 l/24h at 4 weeks postpartum, suggesting that the current iodine status may have been underestimated. The WHO UIC of 150 µg/l during pregnancy and 100 µg/l during lactation at an average of 1.5 litres urine/24 hours translate to estimated cut-off values of 225 and 150 µg iodine/24 hours, respectively. When compared with these, our median iodine excretions at 20 GW, 36 GW and 4 weeks postpartum of 210, 304 and 157 µg/24h, respectively, still suggest inadequacy at 20 GW (i.e. prior to supplementation), adequacy at 36 GW and borderline adequacy at 4 weeks postpartum (during supplementation). In addition, Dold et al.23 recently suggested that maternal UIC alone is not an accurate biomarker of iodine status in lactating women and that additional measurement of BMIC could be useful in the assessment of the iodine status of lactating women.
Notwithstanding possible confounders, we remain concerned about the current findings, given the observation that 61% of the women already took iodine-containing multivitamins prior to the start of supplementation. Maternal iodine needs are higher during pregnancy and lactation because of iodine losses by transplacental transport, the necessity to maintain increased maternal thyroid hormone production, and the secretion of iodine into the milk.5 At least three studies showed an association between a mild to medium iodine insufficiency during pregnancy and a lower IQ of the offspring at 3, 8 and 9 years of age.24-26 For instance, 8-year-old children born to mothers with a urinary iodine/creatinine ratio < 150 µg/g in the first trimester, had higher chances of having a verbal IQ (odds ratio: 1.58), reading accuracy (odds ratio: 1.69) and reading comprehension (odds ratio 1.54) in the lowest quartile,25 compared with counterparts of mothers with a urinary iodine/creatinine ratio > 150 µg/g in the first trimester.
Most,14,20,22 but not all,19 studies showed positive correlations between iodine dosage and the UIC during pregnancy and lactation. We found a trend, probably due to the small number of participants and therefore lack of statistical power. However, the daily supplemental intake of 150 µg iodine did increase the median UIC from 102 µg/l at 20 GW to 144 µg/l at 36 GW. This increase is in line with previous data from pregnant women in two cross-sectional studies conducted in Belgium18 and Austria,22 where supplementation with 150 µg/day also increased the median UIC. However, analogous to our study, they found this dosage to be insufficient to reach a median UIC of > 150 µg/l during pregnancy. At 4 weeks postpartum the median UIC was 112 µg/l. This decrease is probably on account of the preferential partitioning of iodine into the breast milk. Taken together, iodine insufficiency seems prevalent and it is unclear whether 150 µg is sufficient to prevent iodine insufficiency during pregnancy and lactation.
One suggestion could be to increase the iodine dose, or initiate iodine supplementation prior to conception. Such regimens may optimise thyroid hormone stores with positive effects on both mother and child.22 Accordingly, both the European Thyroid Association and the American Thyroid Association guidelines currently advocate to start iodine supplementation prior to conception.27,28
The median BMIC was 1.2 µmol/l (range: 0.5-3.0). Of the infants, 33% had an estimated iodine intake below the IOM-AI (i.e. 1.1 µmol/l) but none had an estimated intake below the Nordic-AI (0.5 µmol/l). Consequently, inadequate infant iodine intake seems less likely. Based on a dose-response crossover study to determine the minimum daily intake of iodine in early infancy, Dold et al.29 suggested a 72 µg/day estimated average requirement and an 80 µg/day RDA for iodine for infants aged 2-5 months. These thresholds are in between those of the IOM and the Nordic AIs and would translate to milk iodine cut-offs at 0.72 and 0.8 µmol/l, respectively. Iodine is concentrated in the lactating breast via preferential transport.30 The milk/plasma ratio amounts to 20-50.31 We did not find a correlation between maternal iodine status and BMIC. Such a relation has been observed,32,33 but not consistently.34,35 In view of the high milk/plasma ratio and the expression of the Na+ /I- symporter in the lactating breast,36 it is likely that iodine is transported preferentially to the infant, and that a marginal iodine status notably occurs at the expense of the mother.
Limitations
This open-label study was not primarily designed to study iodine status and the effect of iodine supplementation. Other limitations are: small study numbers, representativeness of the Dutch pregnant population, day-to-day variation of the UIC, lack of a control group, and absence of information on dietary intake. It must, however, be noted that most of the women in the current study were highly educated and had above average incomes. Most of them used an iodine-containing multivitamin supplement prior to the study start. The RIVM found a positive relationship between education level and iodine intake from natural sources.12 Consequently, the currently studied mothers might have had a better iodine status than the Dutch general population. Information on dietary intake could have improved insights into iodine sources. Other limitations are that we estimated infant iodine intake by using average infant daily milk consumption and that we did not verify the iodine content of the supplements. Conceding the above limitations, but strengthened by similar findings in surrounding countries, we consider the results too worrying to refrain from a report. There is an urgent need to conduct a larger study aiming at the iodine status of a representative group of pregnant and lactating Dutch women.
CONCLUSIONS AND RECOMMENDATIONS
This pilot study suggests a high prevalence (83%) of iodine insufficiency during pregnancy. The insufficiency was not entirely corrected by the use of a daily 150 µg iodine supplement. Due to the potentially severe and easily preventable consequences of iodine insufficiency for both mother and her offspring, a larger and representative study is urgently needed.
ACKNOWLEDGEMENT
We thank Eline Hemelt, Emar Vogelaar, Herman Velvis en Wietske Hemminga for their participation in this study. This work was supported by the Ministry of Economic Affairs, the Province of Drenthe and the Province of Groningen. The supplements were kindly provided by Omega Pharma and Bonusan.
There are no conflicts of interest to report.
REFERENCES