KEYWORDS
Barriers, daily haemodialysis, education, home haemodialysis, nocturnal haemodialysis
INTRODUCTION
In 1961 home haemodialysis (HHD) was introduced by the Japanese doctor Yukihiko Nosé.1 The reason to perform haemodialysis (HD) in this unorthodox environment was primarily a practical consideration, since a proportion of the patients with end-stage renal disease (ESRD) could not be offered in-centre chronic haemodialysis due to capacity problems. The first HHD session was performed by a domestic washing machine with a frame coil dialyser, hence reducing costs. In the early 1960s, HHD programs were initiated in Seattle, Boston and London, and the rest of the world followed shortly thereafter.2
In the Netherlands, the first patient was treated with HHD in 1968.3 In the early 1970s, 59% of the dialysis population in the United Kingdom and 32% in the USA received HHD. By the end of the 1970s the number of HHD patients reached its peak.4 Prevalence in Australia and New Zealand was as high as 45%.5 At that time, 10% of dialysis patients were treated with HHD in the Netherlands.6 Due to several factors, HHD rapidly waned from practice in the 1980s and 1990s, although large variations between countries remained. Australia and New Zealand maintained the largest population of HHD patients (9% and 18%, respectively),7 while prevalence of HHD in the USA declined to 2%8 and some countries no longer offered HHD at all.9 Reasons for the decrease in HHD in the Netherlands include the introduction of continuous ambulatory peritoneal dialysis in 1979,10 the increase of living kidney transplantation, the formation of satellite HD facilities, and eventually, lack of experience of nephrologists.4,11
Over the past decade, cumulative evidence demonstrated improved clinical outcomes with more frequent and/or prolonged (nocturnal) HD (in this paper designated by the term intensive HD), more easily provided in the home environment, compared with in-centre conventional HD (CHD). This, combined with the demand for reduction in healthcare costs, has led to a renewed interest in HHD. In the Netherlands, the number of HHD patients is steadily increasing from 112 (~2.0% of all dialysis patients) in 2006 to 273 patients (~4.2%) in 2016.12 Probably, a lot more patients could benefit from this treatment modality. This narrative review aims to provide a thorough overview of current practices and literature on HHD.
PATIENT SELECTION ,EDUCATION AND TRAINING
Patient selection
Whether a patient is suitable to perform HHD is largely dependent on patient motivation and the availability of family or medical staff support.13,14 In fact, most of the patients requiring dialysis are medically suitable for HHD.13,15,16 According to the National Institute for Health and Care Excellence (NICE), suitable candidates for HHD should be able and willing to learn the technique, be able to carry out the procedure (or be supported by a caregiver), be stable on dialysis, have suitable vascular access and have appropriate housing – after adaptations have been made – to accommodate the HD machine and equipment. Contraindications include severe intradialytic hypotension17 and unstable behavioural problems.17,18 The patient selection process, which includes providing information and a comprehensive assessment of the patient’s healthcare needs and social circumstances including a home visit, should identify patients who are both physically and mentally able to perform HHD.
Patient education
The early identification of a potential HHD patient and timely initiation of patient education in the pre-dialysis period can help to overcome the barriers to HHD (see Barriers to home haemodialysis, later in this article). A comprehensive pre-dialysis education (CPE) program should provide patients and their family with clear and objective information on chronic kidney disease and the different treatment modalities, including kidney transplantation and conservative care. The program should promote self-care dialysis, use a multidisciplinary approach (nephrologist, dialysis nurse, dietician, psychologist, social worker), address psychosocial attitudes, misconceptions and fears, and promote shared-decision making. Of utmost importance is a dedicated team, with expertise in different treatment modalities. CPE programs meeting these criteria are successful in increasing the number of patients choosing home dialysis, including HHD, even after an urgent unplanned start of dialysis.19-21 Shukla et al. reported on a successful CPE program in their clinic for future dialysis patients. The program required patients to attend a half-day at the clinic, starting with a whole-group session on kidney disease and renal replacement therapy options followed by individualised sessions with a dialysis nurse, a dietician, a social worker and the nephrologist. Patients were able to re-attend the program, yet almost 50% attended only one day prior to their first dialysis session. After multiple program meetings, the majority of 70% chose dialysis treatment at home: 55% chose peritoneal dialysis and 15% chose HHD.21 After initiation of the CPE program the number of home dialysis patients more than doubled.
Patient training
Initial HHD patient training is performed by a few training facilities in the Netherlands, since a centralised program facilitates logistics and optimises clinical expertise.22 The training comprises all aspects of HD, from preparation of the dialysis fluid to machine set-up, from access puncturing and access care to assessing dry weight, etc. The training program should train patients and family caregivers to act appropriately in case of acute events and instruct them to call the dialysis centre or hospital 24 hours a day for any acute problem. The training period generally lasts 6-12 weeks, subject to the patient’s knowledge and skills.
PRACTICAL AND TECHNICAL ISSUES
Not every house is suitable for HHD because it requires space, plumbing and electrical modifications to accommodate the dialysis machine, and will put higher demands on standard utilities and services.
Drinking water
The Water Supply Act in the Netherlands sets the standard for water used for drinking, cooking, and other domestic purposes.23 With regard to public health, additional demands are imposed by the ‘drinking water decree’.24 The drinking water regulations establish the standards to be met by water supply companies concerning the design of facilities, control measures, and registration in logbooks.25 The Dutch water supply companies are responsible for the delivery of drinking water that complies to the aforementioned obligations. Dutch drinking water is non-chlorinated and free of chloramines, in contrast to drinking water in many other countries where disinfection with chlorine is still utilised. Chlorine is harmful to reverse osmosis (RO) membranes in the dialysis machine, also chloramines are toxic to humans. In situations where dialysate was contaminated with chloramines, patients developed haemolytic anaemia and methaemoglobinemia.26 If feed water contains chlorine and/or chloramines, an activated carbon filter is mandatory. Because of the non-chlorinated drinking water, activated carbon filters are not a standard feature in water treatment systems for HHD in the Netherlands.
Water treatment systems for HHD
Drinking water taken from the urban supply is not safe for use in HD. Drinking water enters the water treatment system through a backflow-preventing device (figure 1). This backflow preventer is installed to prevent pollution of the urban water supply infrastructure due to backflow of the domestic water system.27
The drawn water passes two coarse filters to remove particulate matter, first a 30-micron sediment filter, then a 5-micron sediment filter. Next, the filtered water may be softened by a softener to protect the reverse osmosis membrane (RO membrane) from calcium and magnesium. The hardness of Dutch drinking water is low. Softeners are thus optional in Dutch domestic water treatment systems. The need for a softener is merely determined by the specifications of the portable RO unit used. Dependent of the brand and type, portable reverse osmose units (RO units) require a water inlet pressure between 1.5 and 3.0 Bar. The water pressure in the Dutch urban water supply systems is sufficient to overcome the pressure reduction by the domestic water treatment system. A booster pump is therefore not a standard feature of the water treatment system at home. Under special circumstances, such as positioning of the water treatment system on the ceiling, a booster pump is needed to provide a water pressure sufficient for normal functioning of the RO unit. The filtered (and softened) feed water is led into the portable RO unit for removal of ions, microbiological contaminants (bacteria, endotoxins, viruses) and dissolved organic substrates.
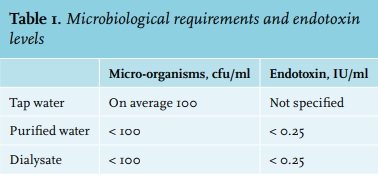
Water leaving the RO unit is called purified or RO water. The RO water is transported to the dialysis machine by a domestic distribution ring adapted to the specific situation on-site. The RO water passes one or two extra filters depending on the specifications of the dialysis machine used, hereby achieving additional bacterial, viral and endotoxin retention. The purified water is further processed into dialysate by adding acid concentrate and bicarbonate. RO water and dialysate for HHD should meet quality standards equal to those specified for in-centre HD as set by The Dutch Federation of Nephrology (in line with the European Pharmacopoeia Commission (table 1)). 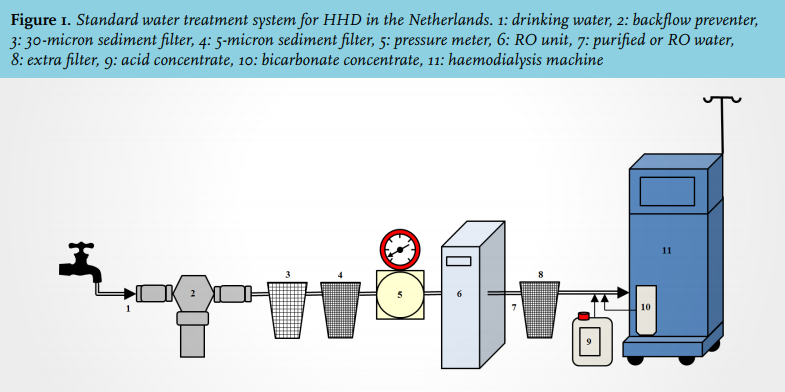
Electrical requirements
The current electrical safety norms, NEN1010:2015, were specified by Academic Hospitals Instrumentation Management Working Group (WIBAZ) in October 2015. NEN1010:2015 was incorporated in the Dutch Building Decree, which entered into force on 23 December 2016. HD is assigned to group 2. Safe HHD thus requires an isolation transformer.
Dialysis machines
Basically, all types of commercially available dialysis machines are suitable for HHD. Differences in design, size, noise level, user interface, and total cost of ownership will guide organisations enabling HHD to opt for a specific brand and type of dialysis machine. Over the last decade, several transportable HD machines have been introduced. They all have a short set-up time with disposable cartridges and automatic priming. These machines have a compact cycler (± 40 x 40 x 45 cm) and make use of 5 litre lactate-based dialysate bags, or have the possibility to produce purified water themselves from the domestic water supply. Novel miniaturised HD machines are in development.
Quality control and maintenance
HHD quality control is organised in accordance with currently applicable clinical guidelines. Quality control includes calibration of the dialysis machine at home at the time of installation, quarterly examination of RO water and dialysate (on bacterial contamination and endotoxins), and a yearly check on the levels of organic and inorganic contaminants. Scheduled maintenance of water treatment systems and dialysis machines is mandatory.
Specific mutual arrangements with water supply companies are necessary. Water supply companies should be informed about patients on HHD in their region and need to inform enablers of HHD timely in case of work on the urban water supply system or increased concentrations of toxic substances, such as aluminium.
Logistics
HHD patients need scheduled home delivery of materials and prescriptions related to dialysis. As a rule of thumb patients receive a four-week delivery, meaning shipment of a trolley containing one and a half to two cubic meters of materials. The materials are to be stored in patients’ homes including an additional two-week stock in case of unforeseen events. Most HHD providers strive for a single supplier situation to prevent frequent deliveries by third parties.
Monitoring of treatment and patients
Monitoring of patients during HHD is an ongoing challenge. So far, monitoring of HHD is based on completed paper records, video calls using available non-secure commercial applications, and/or visits to the outpatient clinic. Initiatives to develop encrypted (safe) IT solutions allowing online monitoring during HHD and video calling and storage of the visual material are eagerly awaited.
HOME HAEMODIALYSIS REGIMENS
The dose of dialysis delivered with CHD is often limited by the overall weekly treatment time and frequency. To deliver the minimum amount of adequate dialysis, CHD utilises high-efficiency dialysis over a short period of time. The resulting peaks and troughs of both hydration status and uraemic retention solute concentrations can lead to dramatic changes in the internal milieu. The home setting offers more flexibility of treatment schedule and facilitates intensive HD sessions, which are summarised in table 2. 28 Intensive HD regimens include short daily haemodialysis (SDHD), prolonged and prolonged-frequent HD. Prolonged (frequent) HD is usually performed during the night (nocturnal HD). Intensive HD can reduce the fluctuations of the internal environment by maintaining a more steady state, and by avoidance of a long interdialytic interval.29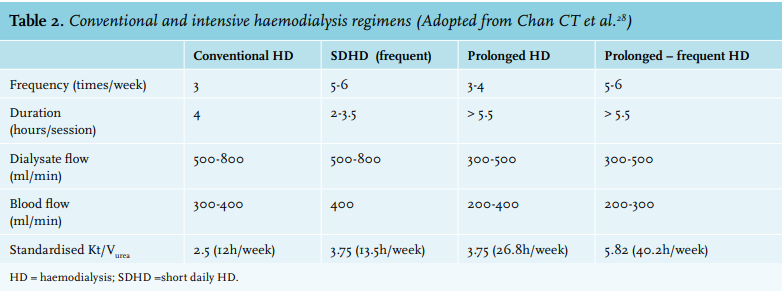
OUTCOMES OF HOME HAEMODIALYSIS
Patient survival
HHD has undergone a significant revival during the past 10 years.30 Growing data supporting the association of intensive HD, most easily achieved in the home setting, with improved outcomes such as survival are the primary drivers for this resurgence. Most survival studies did not compare HHD versus in-centre HD, but intensive regimens (mostly performed at home) with a conventional (3x/week) regimen. Charra et al. reported a dramatic improvement in survival of dialysis patients in Tassin (France) by extending the length of HD sessions.31 The survival benefit for patients undergoing nocturnal (NHD) and short-daily (SDHD) haemodialysis has been evaluated in a number of studies. Although no well-powered randomised controlled trial has been performed to date and the bulk of the data remain observational, the evidence points toward a better survival for patients receiving SDHD and NHD compared with those treated with conventional regimes.32-41 A cohort study by Lacson et al. reported a mortality benefit for in-centre nocturnal HD (INHD) with a significant hazard ratio (HR) at both 1 year (HR 0.73, 95% CI 0.56-0.96, p = 0.02) and at 2 years (HR 0.75, 95% CI 0.61-0.91, p = 0.004) compared with a propensity-scorematched in-centre CHD arm.40 Ok et al. also demonstrated a one-year survival advantage favouring INHD over CHD (HR 0.32, 95% CI 0.10-0.98, p = 0.04) after adjusting for age, gender, dialysis vintage, and the presence of diabetes.41
In a study of prevalent Canadian patients, Pauly et al. reported a five-year survival rate of 85% among patients receiving nocturnal HHD (NHHD), a rate comparable with that of patients who had received a deceased donor transplant in the USA.42 The Frequent Hemodialysis Network (FHN) Nocturnal Trial, randomising dialysis patients to either CHD (home or in-centre) or NHHD (six times a week), did not find a significant effect of NHHD on outcome.43 The lack of differences in the latter trial is likely due to the small number of patients enrolled, an increased number of incident uraemic patients enrolled (> 50%) whose residual kidney function could likely have blunted the beneficial effects of the frequent dialysis, a remarkably low mortality rate in the CHD group, and the fact that one-third of the NHHD patients were less adherent to the treatment with less than 80% of the prescribed dialysis sessions done. Johansen et al. compared intensive (both nocturnal and frequent) HHD with in-centre CHD, using propensity score matching, and reported an HR of 0.36 (95% CI 0.22-0.61) for death, favouring NHHD. SDHD was not associated with a survival advantage (HR 0,64, 95% CI 0,31-1,31).38 The FHN Daily Trial, randomising dialysis patients to in-centre SDHD (six times a week) or in-centre CHD, found a survival benefit in the SDHD treatment group.44 A recent observational study in a large cohort of Canadian HHD patients did not find a reduction in the relative risk for the composite of death and treatment failure in patients treated with either NHHD or SDHD, after multivariable adjustment for patient and centre factors (e.g. vascular access type), compared with home CHD (NHHD: HR 0.83, 95% CI 0.66-1.03; SDHD: HR 0.84, 95% CI 0.63-1.12).45 This could be explained by low mortality rates in all home dialysis groups. Although this study did not demonstrate a benefit of dialysis intensity, potential advantages of treatment in the home environment could not be studied due to the lack of an in-centre treatment group.
Summarising, evidence is growing for improved survival from intensive forms of haemodialysis (frequently but not invariably performed at home), as compared with conventional HD (mostly performed in-centre).
Blood pressure
Blood pressure (BP) control is one of the most consistent benefits of intensive HD in randomised and non-randomised studies.43,46-51 One of the first reports of improved BP control in intensive HD came from France, where mean ambulatory BP was shown to be inversely correlated with HD session duration.52 Subsequently, the FHN study showed a significant reduction in systolic BP of -9.7 mmHg (range from -16.9 to -2.5) during 12 months of follow-up in the NHHD cohort, with a significant decrease in the number of antihypertensive agents.43 The lack of significant difference in BP readings in patients on a CHD prescription (4 hours, 3 times a week) although performed in the home setting, illustrated the importance of intensive HD as opposed to location of HD delivery as the main factor driving BP control. NHD reduces BP by lowering of total peripheral resistance and plasma norepinephrine levels.49,50 Another factor leading to improved BP control is improved fluid balance, as achieved by SDHD.48
Cardiac indices
Evidence from studies with SDHD44,48,53 and N(H) HD46,48,54 demonstrated that intensive HD is associated with improvements in left ventricular mass index and left ventricular hypertrophy, which are factors associated with cardiovascular morbidity and mortality in dialysis patients including heart failure and sudden arrhythmic death.55 These findings are confirmed by a recent meta-analysis of observational studies and data from RCTs that reported improvement in left ventricular mass index and geometry in both frequent and prolonged HD groups.56 Furthermore, a cross-sectional study demonstrated that intensive HD regimens (home or in-centre) were associated with a significant reduction in intradialytic systolic hypotension and dialysis-induced myocardial stunning compared with in-centre CHD.57 A Dutch randomised cross-over study recently confirmed improvement of haemodynamic (peripheral systolic, peripheral diastolic and central BP) and cardiac stability, associated with better preservation of relative blood volume, during prolonged haemodialysis sessions as compared with CHD sessions.58 Finally, two retrospective observational Canadian studies showed that frequent NHHD is associated with improvement of electrocardiographic features linked to sudden cardiac death.59,60
Elimination of the long (2-day) interdialytic interval over the weekend, inherent to a thrice-weekly dialysis regimen, may be an important factor in reducing cardiovascular risk with intensive HD since fluid overload and metabolic derangements (e.g. hyperkalaemia) are more pronounced after the long interdialytic interval and may lead to cardiovascular events and mortality.61-63 Evidence from retrospective observational studies with in-centre CHD suggest that myocardial infarction, dysrhythmia, heart failure, stroke and all-cause mortality (including sudden and cardiac death) are higher on the day after the long interdialytic interval than during any other day of the week.64-69 This pattern was not observed in patients receiving in-centre CHD > 3x/week, HHD (~70% performed dialysis thrice weekly for > 4 h per session and ~20% > 3x/week) or peritoneal dialysis.65 However, an observational cohort study using the US Renal Data System did not find a reduced risk of arrhythmia-related hospital admissions for daily HHD patients as compared with matched in-centre CHD patients. Of note, the risk of heart failure-related admission was ~40% lower.70 Prospective, preferably randomised, trials are required to determine whether intensive (H)HD reduces sudden cardiac death, cardiovascular morbidity and mortality in HD patients.
Bone mineral metabolism
The cumulative evidence points towards improved management of bone mineral abnormalities by the use of intensive HD.43,56,71 It is common for patients on intensive HD prescriptions to require fewer phosphate binders, and they frequently need phosphate supplementation in the dialysate.72 In the long term, improved control of hyperphosphataemia and secondary hyperparathyroidism by intensive HD may translate into significant risk reduction of vascular calcification, potentially contributing to increased survival in this dialysis population. Up to now, data regarding vascular calcification in HHD are inconclusive.73
Anaemia control
Normochromic (renal) anaemia and iron deficiency anaemia are extremely common in the dialysis population.74 It is unknown whether intensive (H)HD has a direct effect on haemoglobin levels or erythropoietin resistance. In observational studies in HHD increased haemoglobin levels were found after intensified treatment.75-77 Yet, an RCT did not find a difference in haemoglobin levels or erythropoietin-to-haematocrit ratio between intensive HD and CHD.54 Evidence from observational studies suggests that erythropoiesisstimulating agent requirement seems to decrease with intensive home treatment,76,77 even in comparison with a propensity-score-matched in-centre CHD arm.78 However, in the FHN nocturnal trial, erythropoietin dosage was not different between the NHHD and the CHD treatment arm.43
Iron supplementation is favoured in the form of intravenous iron, as a better effect on haemoglobin levels is expected.79 However, intravenous iron administration at home is controversial, as serious adverse events (e.g. anaphylactic reactions) might occur.80 This might be a logistic barrier to perform HHD. The Dutch Federation of Nephrology has therefore developed a practical standard for intravenous iron administration at home. Recommendations include administration of a limited amount (maximal 100 mg each time) of non-dextran iron (less known for adverse events) in no less than 30 minutes, by trained patients or nurses with uncomplicated single administration in a centre as prerequisite.81
Pregnancy outcomes
Another important benefit of intensive HD is its effect on fertility. Conception rates and pregnancy outcomes are overall poor in patients on dialysis. There are emerging observational data from patients on intensive HD with lower urea levels that show significantly better pregnancy outcomes compared with CHD.82-85 It is thought that the increased rates of successful conception observed in child-bearing age female ESRD patients receiving intensive HD may be partially due to restoration of the pituitary-hypothalamic axis augmented by improved solute clearance. At the same time, improved clearance (lower urea levels), fluid balance, BP control and haemodynamic stability in intensive HD, could positively impact on pregnancy outcomes.85,86 In the male population, intensive HD (NHHD) could also improve fertility, possibly by an increase in testosterone levels and decreasing hyperprolactinaemia.87
Quality of life
The impact of home intensive HD on quality of life (QoL) has been the subject of multiple studies, and overall results show an increase in kidney-specific domains of QoL parameters.47,54,88-91 This increase in QoL with intensive HD regimes may be due to increased autonomy and functionality, reduced pill burden, liberalisation of dietary restrictions and fluid intake, considerable reduction in the time spent in the hospital and in transit to and from the hospital, optimised employment (productivity), and a reduction of inflammation and uraemic symptoms.
NHHD has been shown to be associated with mood improvement, an important domain of QoL associated with improved outcomes.54 This might be due to improved sleep quality due to a reduction in sleep apnoea with NHHD. The FREEDOM study showed a reduction in the prevalence of restless legs syndrome from 35 to 26% after 12 months of home SDHD (p = 0.05),92 while NHHD has been associated with a reduction in the frequency of sleep apnoea episodes.93
VASCULAR ACCESS
Type of access
A well-functioning vascular access is of crucial importance for safe and long-lasting HHD. According to the European Best Practice Guideline on vascular access,94 an autogenous arteriovenous (AV) fistula is the vascular access of choice in all HD patients. As fear of self-cannulation is the most frequently reported barrier in HHD,95 a central venous catheter (CVC) might be considered to be a suitable type of access for HHD. However, in the in-centre HD population CVC use has been associated with a higher risk of death.96 Of course, this could be explained by differences in patient type between patients with an AV fistula vs. CVC (confounding by indication). However, equivalent results can be found in recent literature in the NHHD and HHD population: patients with CVC treated at home have a higher mortality risk compared with patients with an AV access,97 even in a propensity-matched cohort.98 In addition, using a CVC was associated with a higher risk for hospitalisation and local infections.98,99 Overall, AV fistulas are the first choice and AV prosthetic grafts are preferred over CVCs.94 CVCs should be reserved for a select group of patients with severe artery disease, severe heart failure, malignancy or anticipated short time to kidney transplantation. Also in elderly patients with limited life expectance, a CVC might be an acceptable choice.100,101
Self-cannulation and buttonhole vs. rope ladder technique
HHD patients performing self-cannulation obtain the highest possible independency. In the Netherlands, patients are trained in less than three weeks with the ‘Tandem-hand’ cannulation: the first week the nurse inserts the needle under physical guidance of the patient, the next week the patient inserts the needle with physical guidance of the nurse, the last week the patient performs the cannulation by himself in the nurse’s presence.102 The buttonhole technique, or constant site technique, was first described in 1977.103 Due to repeated insertion of the needle at exactly the same site and in the same angle, in 2-3 weeks’ time a tunnel of fibrous tissue is formed allowing successive insertion with blunt needles. In daily practice, the buttonhole technique is frequently used in patients with fear of self-cannulation since this technique is believed to be less painful. Yet in the HHD literature no significant effect on cannulation pain was found with the buttonhole technique,104 although this study is likely biased since it included a selection of patients experiencing painful cannulation. A definitive advantage is improved survival of AV fistulas, including a reduction of aneurysm formation and reduced need of access interventions, with buttonhole instead of the rope ladder technique.105-107 The biggest concern with buttonhole remains the risk of infections: in a systematic review more infections were found in the buttonhole group compared with rope ladder cannulation (combined RR 3.18, 95% CI 2.12-4.77).108 In conclusion, rope ladder is the preferred method for cannulation. Yet, in patients with a short fistula and fear of self-cannulation, buttonhole remains a possible alternative if preventive hygiene is strictly followed.109
Surveillance
In HD in general, recommendations for access surveillance comprise access flow measurement at least every month in AV grafts and every 3 months in AV fistulas,94,110 and there is no reason to deviate from these recommendations in HHD. Frequent monitoring reduces the risk of thrombosis formation.111 As a routine measure, physical examination prior to any cannulation is recommended in order to identify possible access problems. Patients should be taught how to recognise infections, aneurysm and stenosis and they might benefit from retraining programs.22,112 The ‘Arm Raise Technique’ is an easy tool used to detect a possible stenosis.113 The biggest challenge in HHD is to incorporate frequent monitoring in the home environment. In some HHD centres, patients are invited to perform in-centre HD once every 2-3 months, in order to perform the access flow measurements. In the Netherlands, access flow measurements are executed at home (personal communication).
Access failure and infections
As previously described, HHD presents many advantages above in-centre CHD, but has possible additional complications.
In the FHN trials, the time to first access event (the composite of vascular access associated hospitalisation, repair and loss) was shorter with SDHD and NHHD compared with CHD (HR 1.76, 95% CI 1.11-2.79 and HR 1.81, 95% CI 0.94-3.48, respectively).114 Of note, buttonhole was associated with a longer complicationfree period in comparison to the rope ladder technique. In the separate (underpowered) FHN studies, vascular access events were seen more frequently during follow-up, yet this was not significant (Daily trial HR 1.35, 95% CI 0.84-2.18 (n = 245)44; Nocturnal trial HR 1.62, 95% CI 0.91-2.87 (n = 87)43). Most importantly, the access failure rate (single outcome) in NHHD and SDHD was comparable with in-centre CHD.43,114 We suggest that double needling might be associated with higher repair risks in these trials on frequent dialysis, yet no studies are available comparing complications in single-access needling (often performed in frequent NHHD in the Netherlands) and double-access needling. A well-founded advice on single versus double needling can therefore not be given. As expected, access failure is dependent on vascular access type: an access failure rate of 0.02-0.16/ patient-years was reported in patients using an AV fistula or graft, whereas the rate in patients with a CVC was higher: 0.48-1.07/ patient-years.99,114-120
The event rate of thrombolysis in HHD ranged from 0.27-1.60/ patient-years in patients using CVC. In patients using an AV fistula no thrombosis was seen during a follow-up of 6 months.121 Due to less exposure to pathogens in hospitals, patients on HHD are believed to be less susceptible to infections. Yet, patients treated with intensive HHD (5-6 sessions weekly) were hospitalised for infection more frequently than in-centre CHD patients.70 Possible explanations for this finding include frequent use of the buttonhole technique, mediocre preventive hygiene, and an association with frequent dialysis. Patients performing NHHD and using the buttonhole technique were three times more likely to develop a vascular access-related sepsis than patients performing CHD.116
OTHER COMPLICATIONS
There is a lack of data comparing HHD events to in-centre dialysis events. Tennankore et al. report the occurrence of technical adverse events and severe events requiring intervention at a rate of 0.16 and 0.038 per 1000 dialysis sessions in a cohort of HHD patients dialysing a median of 5 times a week and 8 hours a session.122 The study by Wong et al. described a life-threatening event rate of only 0.060 per 1000 dialysis sessions.123 Thus, current literature indicates that the overall event rates for these complications are acceptably low, which confirms the safety of HHD, but the potential for life-threatening events warrants discussion.49,124 These specific complications relate to three main areas: 1) dialysis techniques; 2) medical factors; and 3) psychosocial aspects.125
Examples of errors in dialysis techniques include machine dysfunction, misuse of dialysis line set, inadequate preparation or contamination of water, and dialysis composition. To prevent technical complications, an adequate education and retraining program for the patient and/or dialysis partner is essential, in addition to accurate protocols and a staff member available 24 hours a day. It is also important to maintain patient awareness of the necessity of these safety protocols.
Successful HHD requires reliable vascular access. Most of the described medical events arose due to AV fistula or graft cannulation needle dislodgements, which were clearly related to patient error or equipment malfunction.122 An unobserved major bleed due to needle dislodgement during nocturnal dialysis is an important possible medical complication. Nevertheless, this risk can be reduced by securing the needles or the CVC with adhesive plasters and by using detector alarms to indicate blood loss. However, in the study by Tennankore, half the patients were not using the offered detector at the time of the event. In the case of nocturnal dialysis, it is possible to reduce this risk by using one needle, with still superior dialysis efficiency compared with a conventional regimen. A few reports address air embolism in the home setting, the majority of which were related to patient error.122,123
Other possible medical complications of HD, including HHD, are hypotensive collapse or cardiovascular instability. However, intensive HHD is also known to be more effective for attaining cardiovascular balance. The safety of NHHD is enhanced by decreasing the ultrafiltration, blood flow and dialysate flow rates. Finally, the medical team should be alert to nutritional deficiencies, especially with regard to phosphate and the water-soluble vitamins. Despite the fact that these vitamins are supplemented after each HD session, we have identified substantial vitamin C deficiency in a significant number of our patients, especially those on intensive HD. Phosphate can be added to the dialysate in the form of phosphate enemas.72
Psychosocial complications are often underestimated, but they influence the endurance of the HHD patient and/ or partner.125 Long-term treatment could lead to anxiety, depression and fatigue because of the perceived ‘gloomy future’ and the demands placed on the patient in terms of time and effort. This may lead to non-compliance and treatment failure. Therefore, psychosocial support is needed before and during the treatment period and the medical team should remain focused on these possible problems.
Thus, several reasons can explain treatment failure in HHD. Recent cohort studies determined that 18-25% of patients discontinued HHD treatment within the first year. Human error is the most common factor contributing to complications arising in the home setting, and usually results from not adhering to prescribed protocols. A high quality and successful HHD program must focus on minimising possible complications, improving event reporting and providing retraining. Therefore, it is important that a dialysis centre offering this modality is experienced in HHD and that patients and staff are trained to detect complications at an early stage. Emergency care for major events should be optimised and in-centre dialysis should be available to patients who fail in HHD. If these factors are considered, the risks for complications are minimal.
BARRIERS TO HOME HAEMODIALYSIS
Despite the benefits of HHD compared with in-centre HD, the majority of dialysis patients (82%) in the Netherlands are treated in-centre with CHD. Both physician- and patientperceived barriers prevent patients from adopting HHD.
Physician attitudes towards HHD are positive. Surveys among nephrologists indicate that there is a strong belief in the benefits of intensive HD and that home is considered the best location for dialysis.126-130 The estimated percentage of patients considered medically and psychosocially fit to perform home dialysis ranges from 15 to 25%,13,18 which exceeds the current proportion of HHD patients in most countries by far. Physician-perceived barriers may, at least in part, explain the discrepancy between physicians’ beliefs in HHD and current practice patterns. The perceived lack of patient motivation is one of the most frequently cited reasons not to start HHD,126,131,132 and may be related to suboptimal pre-dialysis patient education programs. Other commonly reported barriers are related to patient characteristics (e.g. age, comorbidities, cognitive impairment, socioeconomic disadvantages), complexity of the dialysis procedure, limited infrastructure (e.g. lack of training facilities), lack of dedicated resources (e.g. multidisciplinary team to educate and support HHD patients), and lack of expertise by nephrologists.126,133 The increased number of vascular access events in nocturnal HHD patients who perform self-cannulation may also play a role.43 Other concerns are related to the costs of HHD. In the Netherlands, health insurers offer standard reimbursement rates for in-centre HD and HHD. This system is a disincentive to dialysis centres supporting patients on more intensive dialysis schedules and providing assistance by a home dialysis nurse, which are accompanied by higher actual costs compared with self-supported home CHD. This could be counteracted by accurate knowledge of the actual costs followed by offering more differentiated reimbursement rates by healthcare providers, more closely related to the actual costs of dialysis care. The DOMESTICO (Dutch nOcturnal and hoME dialysis Study To Improve Clinical Outcomes) study group aims to conduct a large cohort study including home dialysis patients, to map actual costs of home dialysis, study examples of good practice and overcome barriers.
From a patient perspective, reasons not to opt for HHD are related to fears and the burden of undertaking HHD. The major barriers perceived by in-centre HD patients are lack of explanation of self-care dialysis, fear of self-cannulation, fear of a catastrophic event in the absence of medical staff support, the burden placed on family caregivers, lack of self-confidence and/or self-efficacy in performing dialysis at home and a coinciding fear of receiving substandard care.134-137 Other reported barriers are a belief that patients should be supervised by medical staff, fear of social isolation, interference of treatment with home life, reluctance to perform the required home adaptations and insufficient space to store equipment and supplies.136,137 Physician and patient perceived barriers have to be overcome to expand HHD practice. Motivation and education of both patients and staff is essential to achieve this.138,139 Specialised training in HHD for nephrologists will create awareness of the benefits of this modality and encourage them to offer this treatment to patients. The characteristics and effectivity of a CPE program were addressed in the paragraph ‘Patient education’. When patients opt for HHD, a patient-tailored plan should be drawn up. Allowing and encouraging patients to perform HHD independently of a family caregiver may enable more patients to adopt HHD and decrease the perceived burden on family members. Experiences from the UK and Finland show that solo-dialysis is feasible for the vast majority of HHD patients.140 The support of a skilled home dialysis nurse may facilitate HHD in the absence of a family caregiver, in the case of debilitated patients or the elderly, who are now often considered poor candidates for HHD, and for patients with a CVC.141,142 Staff-assisted HHD eliminates the need for patient training and can be initiated immediately after installation of the equipment at home. It increases the patient’s confidence in HHD and motivates patients to take responsibility and start a training program for self-supported HHD. The experience of a Dutch dialysis unit with 10 years of staff-assisted HHD shows that 30% of the patients starting with staff-assisted HHD can be converted to solo-dialysis or family-supported HHD (personal communication). Also, a hybrid of staff-assisted HHD and self-assisted HHD can be applied. For instance, when a patient and partner are afraid of self-puncturing, but can be responsible for the dialysis procedure, a skilled dialysis nurse can simply do the puncturing for them. Last, the design of less complex HHD devices requiring less storage space and less home modifications and the application of remote monitoring technology143,144 may improve patients’ confidence to perform dialysis independently and effectively without direct supervision of medical staff, and in addition may shorten time of HHD training programs and lower the costs.
NEW DEVELOPMENTS
The increased popularity of HHD has stimulated the development of less complex, transportable (24-34 kg) and more user-friendly dialysis machines (see dialysis machines).145,146 All of these machines are low-dialysate-flow systems (max 300 ml/min) requiring an increased time on therapy (typical treatment scheme: 4-6 times per week 2.5-4 hours). In the near future the release of a new compact (45 x 37 x 48 cm) cartridge-based dialysis machine of 29 kg suitable for HHD is expected (not yet FDA approved or CE certified).147 The device needs a domestic water treatment system, but dialysate flow rates up to 500 ml/min can be applied.
The weight of the transportable HD machines is still considerable (≥ 24 kg) and all systems rely on conventional technology using pre-mixed or in-situ mixed dialysate (≥ 20 litres per treatment) in a single pass configuration. Continuous regeneration and reuse of a small amount of dialysis fluid in a closed-loop system renders the system independent of a large dialysate supply and allows further miniaturisation, but the technology is challenging. Currently, a portable artificial kidney of ~10 kg using ~6 litres of dialysate, is being developed by a collaborative effort of the Dutch Kidney Foundation and several biotechnology companies, based on the REDY (REcirculation DialYsis) technology combining adsorbent, ion exchange and enzyme techniques.148 The device will be designed for every-other-day HHD. A functional model became available in 2016 and a first in-human clinical trial is expected to start in 2019. Other companies are working on comparable sorbent HD systems.149,150 In the meantime, initiatives towards further reducing the dimensions to wearable proportions, allowing maximum flexibility for the patient, are ongoing. One of the major challenges is urea removal since direct adsorption of urea is very difficult while a relatively large amount needs to be removed daily (around 400 mmol ≈25 grams).151 A wearable artificial kidney of 5 kg relying on urease (as the REDY technology) has been designed. Urease is an enzyme that catalyses hydrolysis of urea to carbon dioxide/bicarbonate and ammonia/ammonium. The device was successfully tested in a first-in-human trial during 24 hours (FDA fast track status).152 However, removal of ammonium, which is more toxic than urea, requires extra sorbent (zirconium phosphate) and solutes (i.e. concentrated infusate with cations removed by zirconium phosphate and sodium bicarbonate to neutralise protons released in exchange for ammonium) which limits further miniaturisation. Initiatives to develop alternative urea removal strategies allowing further miniaturisation to truly wearable proportions (< 1.5 kg) such as direct adsorption153 and electrochemical urea degradation154 are ongoing but still far from clinical application.
Another development in the field of HHD is the application of remote telemonitoring systems to record patient- and treatment-related parameters and allow for (face-to-face) communication.155,156 This could reduce patients’ experiences of social isolation and anxiety about the absence of medical staff, reduce travel time and enable health professionals to monitor treatment and compliance more continuously, advise patients on how to adjust their treatment themselves, and facilitate remote assistance in case of acute problems.
The Dutch Kidney Foundation is supporting some of these new developments, and also stimulates the different forms of home dialysis by the recent initiation of a Taskforce Home Dialysis.
CONCLUSION
It is difficult to make practice recommendations regarding HHD based on the current body of evidence. There is a lack of large RCTs, which are not feasible to perform. Well-matched prospective cohort studies on a broader range of outcomes (e.g. quality of life, hospitalisations, vascular access associated complications, blood pressure control) are needed to provide greater certainty about the clinical benefits of HHD. However, current evidence indicates that intensive HD, facilitated in the home setting, is associated with improved clinical outcomes at the expense of more vascular access complications. Although severe and life-threatening events rarely occur in HHD, strict regulations combined with patient education and retraining on technical issues, preventive hygiene and emergency situations are important. In order to provide a high level of care, in both knowledge and logistics, a dedicated and experienced team is needed. National initiatives to promote learning between centralised dialysis facilities and regional centres are currently in development in the Netherlands.
DISCLOSURES
The Dutch Kidney Foundation supported the work of A.A. Bonenkamp, M.K. van Gelder and K.G.F. Gerritsen. A.C. Abrahams, B.C. van Jaarsveld, A. van Eck van der Sluijs and A.A. Bonenkamp are involved in the DOMESTICO study.
The authors have no conflicts of interest to declare.
REFERENCES