KEYWORDS
Granulomatous disease, hypercalcemia, pancreatitis, sarcoidosis.
INTRODUCTION
Sarcoidosis is a granulomatous disorder that usually occurs in the lungs (90%) and lymph nodes, although other organs can be affected. Pancreatic involvement in postmortem examinations ranges between 1 and 5%1 and clinically apparent pancreatitis has been described sporadically in separate case reports.2-7 To our knowledge, only four cases of sarcoidosis presenting as pancreatitis have been reported.4-7 In all cases pulmonary sarcoidosis was also present. We report the case of a female patient without pulmonary sarcoidosis who presented with hypercalcaemia and acute pancreatitis which resulted from extensive abdominal sarcoidosis.
CASE REPORT
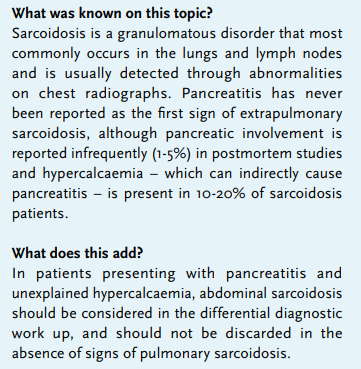
A 60-year-old woman with a psychiatric medical history presented to our emergency ward with a decreased level of consciousness (Glasgow Come Scale, E3M3V5), hypoxia, tachycardia and pain in the upper quadrants of the abdomen. Laboratory examination showed hypercalcaemia (3.24 mmol/l, corrected for albumin levels (32 g/l)), elevated amylase levels (1859 U/l), acute kidney injury (creatinine 393 µmol/l), increased inflammatory parameters (CRP 86 mg/l; leucocytes 19.5x109/l) and elevated lactate levels (2.8 mmol/l). Computed tomography (CT) of the abdomen showed signs of acute pancreatitis with extensive abdominal fluid collections and reactively enlarged lymph nodes (figure 1A). The patient was admitted to the ICU for intravenous fluid suppletion. We proceeded with further evaluation of the hypercalcaemia. Parathyroid hormone (PTH) and 25-OH vitamin D levels were low, while 1,25-OH vitamin D level was elevated (table 1). Vitamin A level was low, free T4 level and PTH-related protein (PTHrP) were normal.
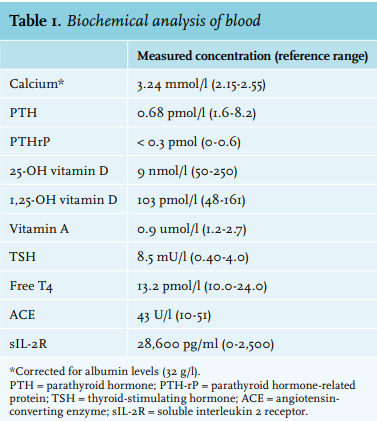
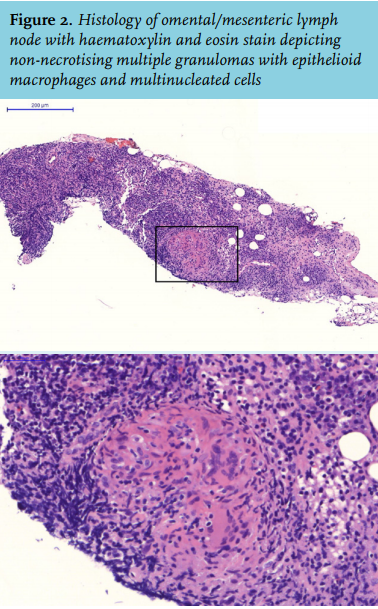
Angiotensin-converting enzyme (ACE) level was normal and soluble interleukin 2 receptor (sIL-2R) was strongly elevated (table 1). CT thorax showed no lymphadenopathy nor pulmonary parenchymal abnormalities. Radiographic studies of the abdomen depicted an inhomogeneous spleen and liver with a thickening of the colon lining, omentum and mesentery (figure 1B-C). Histology of a lymph node left of the middle line of the stomach revealed a non-necrotising granulomatous inflammation with no evidence for acid-fast or other organisms (figure 2). Histology cultures were negative for tuberculous and non tuberculous mycobacteria. We thus diagnosed abdominal sarcoidosis, with evidence of involvement of the liver, spleen, and omental/mesenteric lymph glands.
During admission, the patient received continuous venovenous haemofiltration (CVVH) for the acute kidney injury, she was resuscitated twice – most likely due to intravascular hypovolaemia – and she developed delirium and pneumonia. Her calcium levels returned to normal after CVVH and her kidney function normalised. Amylase levels and inflammatory parameters returned to normal and she fully recovered clinically.
Therapy with prednisolone was initiated (2 weeks 30 mg/ day followed by 4 weeks 20 mg/day) after discharge from the hospital. Albumin-corrected calcium levels decreased from 3.39 mmol/l to 2.62 mmol/l in the first month of treatment. The calcium levels remained stable under low-dose prednisone treatment and the sIL-2R levels decreased significantly (6804 pg/ml after 4 months of treatment). 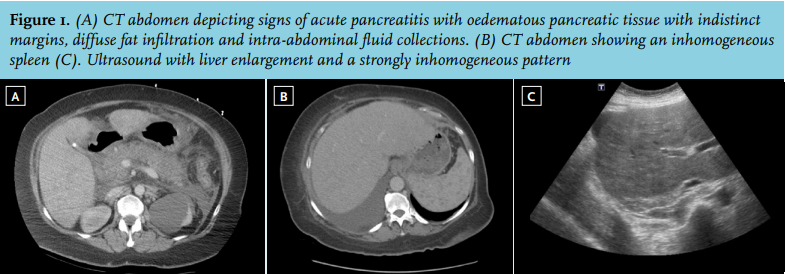
DISCUSSION
We report a patient who presented with acute pancreatitis due to sarcoidosis. The acute pancreatitis in our patient may have been secondary to the hypercalcaemia – by activation of trypsinogen by calcium deposition in the pancreatic duct8 – or caused by pancreatic granulomatous infiltration leading to inflammation and obstruction of pancreatic drainage.2 Seven cases of pancreatitis in sarcoidosis have been described previously in which all but one3 had concomitant hypercalcaemia. About 10-20% of patients with sarcoidosis have hypercalcaemia, due to increased intestinal calcium absorption driven by 1,25-OH-vitamin D.9 In sarcoidosis, 1α-hydroxylase produced by activated mononuclear cells stimulates PTH-independent conversion of 25-OH-vitamin D to the biologically more active 1,25-OH-vitamin D and its activity is further enhanced by inflammatory factors.10 Clinically apparent pancreatic sarcoidosis is extremely rare and besides presentation with acute pancreatitis could also present with a mass in the pancreas or a diffusely firm nodular pancreas.1 No signs of pulmonary invasion of the sarcoidosis were present in our patient. In all known cases (n = 7, to our best knowledge) of sarcoidosis with pancreatitis the lungs were also affected.2-7
Serum ACE levels were normal in our patient and sIL-2R was strongly elevated. With treatment of the sarcoidosis, the sIL-2R levels strongly decreased. sIL-2R is more sensitive for sarcoidosis compared with ACE (sensitivity in literature: 79-98% vs. 22-73%), especially for non-pulmonary sarcoidosis, and can be used in the diagnostic work-up.11-13 However, both parameters lack specificity.11-13 Therefore, for the diagnosis of sarcoidosis, histopathological detection of noncaseating granulomatous is essential. Radiographic evaluation can aid to determine an accessible biopsy site. Additionally, sIL-2R has potential as a marker for disease activity, especially for non-pulmonary manifestations.12,13
In conclusion, acute pancreatitis can be a presenting symptom of sarcoidosis, although it appears to be extremely rare. Therefore, sarcoidosis should be considered a cause of acute pancreatitis, even in the absence of more common organic involvement such as pulmonary sarcoidosis, and especially when there is evidence of hypercalcemia.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES