KEYWORDS
Elderly, geriatric assessment, rehabilitation, geriatrician
INTRODUCTION
Geriatric rehabilitation care is provided at nursing homes for older persons who temporarily suffer from functional decline due to a variety of medical reasons, with the intention to return to independent living after recuperation. It comprises an active form of care, offered on specifically equipped wards by a multidisciplinary team.1,2 Geriatric rehabilitation care is available after hospitalisation, for instance after hip fracture or pneumonia; however community dwelling elderly patients can also be referred by their general practitioner (GP) in case of a decline in self-reliance due to an acute-onset condition.2,3
Originally, geriatric rehabilitation care was provided under the Exceptional Medical Expenses Act (AWBZ). However, as this type of multidisciplinary care is more complex and expensive than long-term nursing care, the financing from the AWBZ was insufficient. Moreover, it did not stimulate short and intensive rehabilitation treatment enough due to fixed day tariffs. Therefore GR care was transferred to the Dutch Health Care Insurance Act (ZVW) in 2013.2 With this change in funding, hospital admission prior to geriatric rehabilitation became a prerequisite in order to recognise and treat all medical conditions needing hospital care. Consequently, this led to unnecessary clinical admissions as not all patients needed hospitalisation.4
In 2014 this practice changed and a hospital admission was no longer a precondition. Nevertheless, as advocated by the Dutch Society of Geriatricians (NVKG),3 a comprehensive geriatric assessment (CGA) performed by a geriatrician prior to geriatric rehabilitation care, to rule out somatic pathology requiring clinical admission and to evaluate geriatric multimorbidity, remained obligatory.5,6
This assessment is incorporated in our regional protocol as an essential precondition before referral for geriatric rehabilitation. The GPs, elderly care physicians and geriatricians in our region are familiar with this arrangement. Thus, the elderly care physicians do not accept patients for admission to a geriatric rehabilitation facility without prior geriatric assessment. Geriatricians perform the assessment on the emergency ward in our general hospital. There is little evidence on the usefulness of this assessment. It may be an unnecessary effort as GP referral directly to geriatric rehabilitation might suffice.
The current study aims to provide insight into this trajectory, by evaluating community dwelling patients referred to our hospital by their GP for geriatric assessment prior to geriatric rehabilitation care. The primary aim is to present the percentage of patients admitted to hospital after CGA, as this shows the number of patients actually needing admission into a cure facility instead of a care facility. Furthermore, the reason for hospital admission, length of stay, new diagnostic findings and advice given to the elderly care physician are described.
MATERIALS AND METHODS
Study design and population
All community dwelling patients referred by their GP to our emergency ward for geriatric assessment before geriatric rehabilitation referral were included in a period of 10 months. Prior to this, the GP already consulted the elderly care physician, who agreed on geriatric rehabilitation care, providing there is no hospital indication, and arranged a bed on a geriatric rehabilitation ward in a nursing home. A CGA is performed in the emergency room by a geriatrician, and depending on the results the patients will go to the nursing home or will be admitted.
Comprehensive geriatric assessment
A CGA has proven to effectively explore the multiple domains of health in elderly patients in many different clinical settings,7,8 among which the emergency department.9,10 It is a diagnostic process, which is used regularly by geriatricians to determine medical, functional, psychological and social capabilities and problems of their patients. All patients underwent a standard diagnostic work up in accordance with the guideline ‘Comprehensive Geriatric Assessment’ by the NVKG.11 It includes a medication review, laboratory tests and relevant diagnostic imaging.
Data collection
For this descriptive study, patients were included consecutively and prospectively between March and December 2016. There were no exclusion criteria. Data were analysed retrospectively. Information of the patient’s status at the moment of presentation was gathered from the patient file, which comprises reason for referral; Charlson Comorbidity Index;12 cognitive impairment; polypharmacy, defined as chronic use of five or more medications;13 hearing and visual impairment; activities of daily living (ADL) and instrumental activities of daily living (IADL) dependency11 and living situation. Data collection was carried out in Castor EDC, a data format which guaranteed anonymity of the patients. The protocol for this study was evaluated and approved by the local ethics committee of the participating hospital.
Endpoints
The primary aim was to determine the percentage of patients that required clinical admission after CGA. We additionally described the reason for hospital admission and length of stay. Furthermore, we collected new diagnostic findings based on the CGA; advice given by the geriatrician to the elderly care physician in the geriatric rehabilitation facility and the rate of admissions to hospital within two weeks after referral for geriatric rehabilitation. Several outcomes were categorised in general groups by three independent researchers; any disagreements were solved by discussion.
Data analysis
Analysis to describe the patient characteristics was performed using SPSS software (version 22). Continuous variables that were distributed normally were displayed using mean and standard deviation. If variables were not normally distributed, the median and IQR were calculated. Categorical variables were displayed with percentages and absolute frequencies. Data were split to visualise the differences between the group with an indication for geriatric rehabilitation care and the group with a clinical admission indication.
RESULTS
Patient inclusion and characteristics
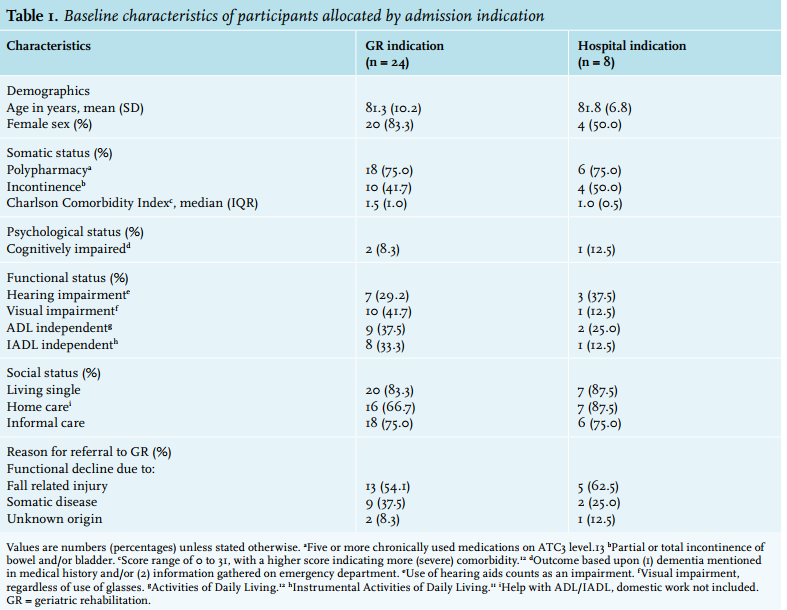
In total, 32 patients were included (figure 1). Table 1 presents the characteristics of patients with an indication for geriatric rehabilitation care and patients who had a hospital admission indication after CGA. Mean age was 81.3 years (SD 10.2) vs. 81.8 years (SD 6.8) for the geriatric rehabilitation and hospital indication groups, respectively. There was a high rate of polypharmacy in both groups at 75.0%. In the geriatric rehabilitation indication group, a higher rate of visual impairment was seen. The majority of both groups received informal care. More patients in the hospital indication group were ADL- and IADL-dependent and received home care. All patients were referred by their GP because of functional decline, primarily due to a fall-related injury, mostly concerning suspicion of hip contusion and backache. 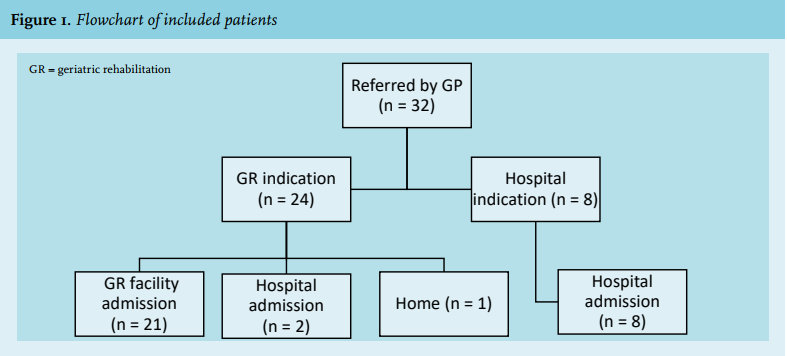
Findings
As shown in figure 1, of all the 32 patients, eight (25.0 %) had an indication for clinical admission. Table 2 shows that six patients required medical treatment, primarily for a respiratory infection or a complicated urinary tract infection. Two needed further diagnostics for suspected neurological disorders, concerning possible cauda equina syndrome and lumbar spinal stenosis. Their average stay was 5.7 days, with a range of one to 12 days. After hospital stay seven patients went to a GR facility, one patient moved to a long-term care facility for elderly with dementia.
Twenty-four patients had a geriatric rehabilitation indication, of which 21 went directly to a geriatric rehabilitation facility. One patient went home, because he refused rehabilitation. Two patients stayed in hospital for one night because no bed was available in the geriatric rehabilitation facility (figure 1).
New diagnostic findings after CGA mainly included infection (four patients with urinary tract infection and two patients with respiratory infection) and fall-related fractures, including vertebral, costal and femur fractures. In the geriatric rehabilitation indication group, the advice given to the elderly care physician concerned management of somatic problems in 75% of cases, e.g. vitamin supplements or treatment of infection or osteoporosis, and often on pain management and drug dosage adjustment. None of the 24 patients with an indication for geriatric rehabilitation were readmitted to the emergency department within two weeks after referral to the rehabilitation facility.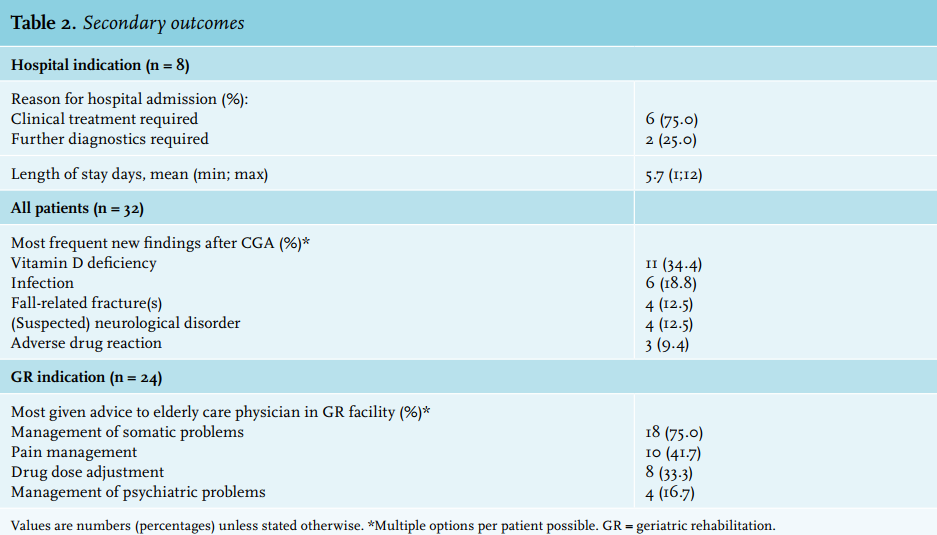
DISCUSSION
We studied the added value of a geriatric assessment in hospital prior to geriatric rehabilitation care. The main finding is that a fourth of all patients referred by their GP for geriatric rehabilitation required hospital admission. Thus, geriatric evaluation prior to referral for geriatric rehabilitation is essential to rule out the need for hospital care. Next, our study shows that the assessment results in important diagnostic findings and useful recommendations for the elderly care physician in the geriatric rehabilitation facility, mostly concerning somatic problems and medication adjustments.
As this specific trajectory to geriatric rehabilitation is based on national legislation, our results cannot be compared with international findings. Also, as far as we know, no previous evaluations in the Netherlands have taken place on this specific issue, namely the community dwelling patients referred by their GP. However, our findings are in line with the expectations of the NVKG,3 who stated that this geriatric evaluation is necessary to select patients in need of clinical care.
As the assessment is performed in hospital, extensive and faster options for diagnostics are available compared with an evaluation in a care facility. It results in appropriate clinical treatment for patients with underlying acute illness. Admission to a care facility will, in all likelihood, cause a delay in treatment. Moreover, none of the patients were readmitted to hospital after referral to a geriatric rehabilitation care facility, which is consistent with prior studies in which a geriatric assessment adequately selects patients with a high risk of readmission.14,15
In two cases direct admission for rehabilitation care was not possible because no beds were available in a geriatric rehabilitation facility. It shows that beds are sometimes available to a limited extent resulting in unnecessary hospital admissions, which leads to additional healthcare costs.
A major strength of the study is that a fixed regional protocol was used to select and refer community dwelling patients to geriatric rehabilitation care, which enabled us to include all patients of our region in the study period.
The present study also has some limitations. It has a rather small sample size and a relatively short study duration. Next, the study was performed in one hospital, thus one region. It is possible that there are interregional differences arising from a different interpretation of legislation, resulting in a slightly different care trajectory.
CONCLUSION
This study shows that current practice is effective. Geriatric assessment prior to geriatric rehabilitation care referral is essential to rule out the need for hospital admission. Also, it results in new diagnosis and relevant recommendations for the elderly care physician in the geriatric rehabilitation facility.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES