CASE REPORT
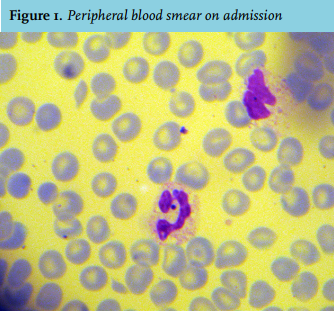
A 69-year-old woman was admitted to the intensive care unit (ICU) with a one-day history of coughing, nausea and drowsiness. She was a profound smoker and drank 3 units of alcohol daily. Medical history revealed myocardial infarction. Known prescribed medications were metoprolol, quinapril, pravastatin and carbasalate calcium. Physical examination showed a respiratory rate of 35/minute, heart rate of 82/minute, blood pressure of 129/62 mmHg and a tympanic temperature of 36.1°C. She had a poor circulation with cold extremities and prolonged capillary refill. We observed a Glasgow coma scale of E3M5V3, no meningism or skin abnormalities; lumbar puncture was not performed because of low suspicion and severe coagulopathy. She had poor dental condition and had recently lost a tooth. Blood gas analysis showed mild respiratory compensated metabolic acidosis (pH 7.47, pCO2 3.6 kPa, HCO3- 19.7 mmol/l, base excess -3.1 mmol/l) and reasonable oxygenation (pO2 9.1 kPa, SatO2 95%). Laboratory results showed a normal haemoglobin level (8.7 mmol/l), leucocytopenia/thrombocytopenia (2.8 x 109/l and 50 x 109/l, respectively), severe coagulopathy (APTT 80 seconds, PT 31 seconds, INR 2.0), C-reactive protein 237 mmol/l, lactate 3.6 mmol/l, creatine kinase 1096 U/l and acute kidney injury with a creatinine of 150 μmol/l. Chest X-ray and CT scan of the cerebrum, thorax and abdomen showed no abnormalities. We suspected sepsis, collected blood cultures and started treatment with broad-spectrum antibiotics according to the hospital protocol (penicillin 12 million units a day, clindamycin 600 mg four times a day and a single dose of 360 mg gentamicin). A peripheral blood smear was also done at admission, as shown in figure 1.
WHAT IS YOUR DIAGNOSIS ?