
KEYWORDS
Nitrous oxide, recreational drugs, vitamin B12 deficiency, hemolysis, neurological impairments
INTRODUCTION
There is an increase in the recreational use of nitrous oxide (N2 O) in the Netherlands.1 Users consider the low costs, wide availability, legal status and quick effect as beneficial.1 A balloon is generally used for inhalation and after one inhalation an euphoric effect can be expected. By public opinion, it is considered a relatively safe drug, but is that joyful moment really innocent? We present a 23-year-old woman with recreational N2 O use who presented to our emergency department.
CASE REPORT
This patient, from Yemeni descent, with a previous history of iron deficiency and recurrent venous thromboembolism, presented to our emergency department with acute paresis of her legs and tingling of her limbs. She had no urinary or faecal incontinence. She was not taking any medication, used alcohol socially and mentioned the recreational use of N2 O multiple times daily. On neurological examination, she had symmetrical weakness of the iliopsoas muscle and quadriceps MRC grade 4, paralysis of dorsal flexors of the feet MRC 0, plantar flexors MRC 3, areflexia of the legs and feet, indifferent plantar reflex response, loss of vibration sense from knees to toes and paraesthesia in both legs.
No abnormalities of the cranial nerves and the arms were observed. Vital signs and general medical examination were unremarkable.
Laboratory analysis revealed a direct antiglobulin test (DAT)-negative haemolytic anaemia: haemoglobin 5.5 mmol/l (7.5-10), leukocytes 1.4 x 109 (4.3-10.0), platelets 266 x 109 (150-400), MCV 98 fl (80-100), vitamin B12 85 pmol/l (130-700), folic acid 36.6 nmol/l (> 5), homocysteine 120.4 µmol/l (3.6-13.0), and methylmalonic acid 1.10 µmol/l (< 0.45).
Electromyography showed axonal polyneuropathy with demyelination. Additional magnetic resonance imaging showed a normal cerebrum and spine. Lumbar puncture revealed no abnormalities in the cerebrospinal fluid, and testing for tuberculosis and polymerase chain reaction for viral infections was negative.
In conclusion, our patient was diagnosed with a non-immune haemolytic anaemia, leukopenia and severe neurological signs as a result of a severe vitamin B12 deficiency due to recreational use of N2 O.
We started treatment with vitamin B12 supplements, folic acid and intensive physiotherapy. After starting the supplements all the laboratory abnormalities gradually normalised but the paraparesis persisted, requiring admission into a rehabilitation centre. After 6 months of intensive physiotherapy and rehabilitation, a slight improvement of the paraparesis has occurred; however, the patient is still only capable of walking within her own home with a walking frame.
DISCUSSION
Vitamin B12 deficiency is a common disease with a prevalence of 5-10% in the Dutch population.2 It is critical to recognise vitamin B12 deficiency since it can cause a demyelinating nervous system disease and bone marrow failure.2 It is associated with a wide variety of signs and symptoms, including macrocytic anaemia, leukopenia, depression, paraesthesia and gait disturbance.1,3-7
Many conditions are known to cause vitamin B12 deficiency such as inadequate dietary intake, atrophic gastritis, celiac disease and malabsorption. One of the more unknown causes of vitamin B12 deficiency is N2O which in the past was used as a relatively safe anaesthetic agent. The recreational use of N2O is rapidly increasing, mainly in clubs and festival scenes, as described earlier by Van Amsterdam et al.1 But nowadays you will also find an increasing amount of discarded N2O canisters (whippets) left on the streets by teenagers. In the age of 12-16 years, 8% have used N20 and 2% had done so in the past month.8 The prevalence increases with age, at 16-18 years one out of six students have used N2O and 20% had done so in the past month.8 The Global Drug Survey 2016 reported that 48.3% of the Dutch respondents had ever used N2O and 33% had done it recently vs. 38% and 23.7% in the United Kindom.9
Inhalation of N2O reduces anxiety and induces euphoria, with a rapid onset with the peak around one minute after inhaling and then fading after 2 minutes.1,10
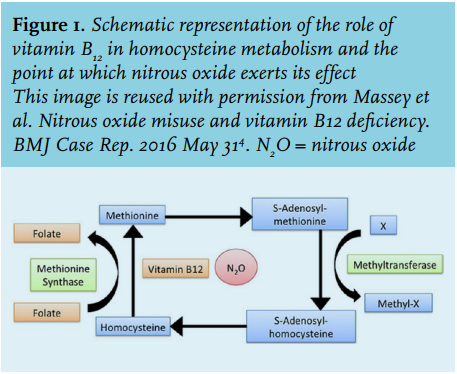
However, the use of N2O is not as innocent as many people think. When N2O is used in high daily doses within a short period or for a prolonged duration, it will irreversibly bind, oxidise, inactivate and eventually deplete vitamin B12 (figure 1).1,4 Several case reports describe vitamin B12 deficiency after repetitive use (50-100 bulbs) of N2O within 3 hours or heavy use over prolonged time, e.g. more than 10-20 bulbs daily for 10 days.1,5 Massey et al.4 describe a myeloneuropathy secondary to vitamin B12 deficiency and Morris et al.11 describe a progressive lower motor neuronal degeneration despite adequate vitamin B12 repletion, suggesting that N2O toxicity on motor nerves may be independent of vitamin B12-dependent metabolic pathways.
Here we report a young female with severe neurological impairments and haemolysis as a result of vitamin B12 deficiency due to recreational use of N2O. With the increase in long-term recreational use of N2O, physicians should be aware of this unknown cause and specifically ask about N2O use when young patients present with vitamin B12 deficiency.
CONCLUSION
This case emphasises the serious adverse effects of nitrous oxide abuse. Secondly, we should be aware that there is an increase in the use of N20 in the Netherlands.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES