KEYWORDS
ABCDE, primary assessment, medical emergencies, emergency department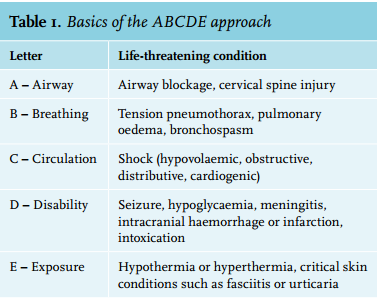
INTRODUCTION
A structured approach is considered a hallmark of the initial care of specific medical emergencies. It facilitates optimal use of time and early recognition of deterioration, especially in the so-called ‘golden hour’ which is the first hour after onset of injury or illness when resuscitation could be most beneficial.1,2 This golden hour has been recognised in various emergencies such as trauma, stroke, sepsis and shock.3-5 The application of a structured approach has become standard in trauma. This approach for early recognition and treatment of life-threatening conditions in trauma has been trained in trauma courses for decades.5,6 Training of a systematic approach using the Airway Breathing Circulation Disability Exposure (ABCDE) primary assessment in other medical emergencies has increased during recent years, although solid evidence of the clinical benefits for patients using the ABCDE approach is lacking. Despite this lack of hard evidence, the Dutch Inspection for Healthcare (IGZ) requires that physicians treating patients in the emergency department are ABCDE trained.7 The scale of transfer to real practice and the extent of the application of a structured approach in the emergency department (do they actually apply what they have learned in training) is not exactly known. The basics of the ABCDE approach are shown in table 1. 8
We have completed an observational pilot study to register the use of the ABCDE approach in the emergency department (ED) in medically ill patients. We investigated whether triage code was associated with performing an ABCDE approach and why a doctor did not deem an ABCDE approach necessary.
MATERIALS AND METHODS
An observational pilot study was conducted in the ED of a tertiary care university hospital with over 34,000 ED visits annually. During a seven-week period from August 2014 until October 2014 a convenience sample was obtained by screening all medical patients older than 18 years admitted to the ED for the internist or emergency physician between 08.00 and 17.00 hours from Monday to Friday on 30 random days. All staff and residents/interns in our ED, except medical students, had to successfully complete a two-day ABCDE course before they could treat patients in the ED. In the Netherlands, there are several of these ABCDE courses provided, consisting of lectures and practical hands-on sessions using simulation. If the attending physician planned to use the ABCDE approach, informed consent was obtained from the patient and physician to observe the procedure. The observer was able to observe/include only one patient at a time. Before assessing the patients, the treating physician was asked which approach he was going to use and the reasons for this specific approach, including reasons for not performing the ABCDE approach. Baseline data were registered including elapsed time until the start of the ABCDE approach, duration of the ABCDE approach, basic patient characteristics (triage code, reason for ED visit) and physician characteristics (physicians and residents were asked about their specialty, duration of current education and years of experience since graduation from medical school). The triage code was allocated by a trained triage nurse based on the main complaint, basic vital parameters and expected amount of resources needed, according to the Emergency Severity Index. This results in five triage codes: red meaning immediate resuscitation needed; orange almost immediate resuscitation needed (within ten minutes); yellow denotes a potentially ill patient with resuscitation needed within one hour, or two or more resources (investigations/diagnostics) needed; green no resuscitation needed but treatment within two hours and only one resource needed and finally blue no resources needed and treatment within four hours. Patients were divided into two groups based on their triage code: red, orange and yellow were grouped together as urgent or (potentially) unstable patients, green and blue as non-urgent or stable patients. Potentially unstable patients can have various serious conditions, for example sepsis, overdose or acute abdominal pain. The ABCDE approach was observed and its completeness was registered using an observational list (figure 1). Completeness scores were calculated by dividing the number of performed checklist items by the total number of checklist items (26) multiplied by 100, resulting in a possible score between 0 and 100. Data collection was performed by one investigator. The study was approved by our local Medical Ethics Committee. 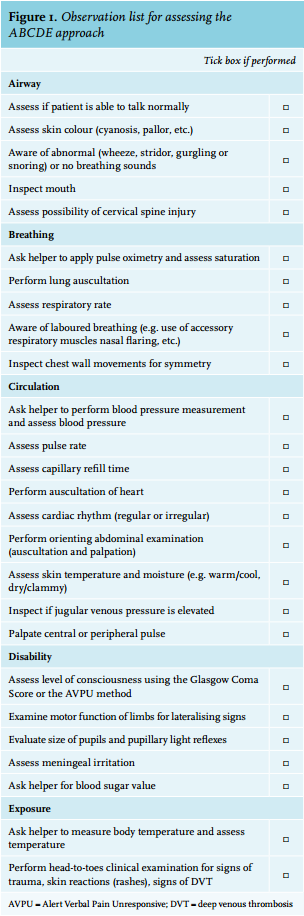
Data analysis
Data were analysed using IBM SPSS version 22.0. A p-value less than 0.05 was considered statistically significant. Descriptive statistics were used. The Jonckheere-Terpstra test was used for the relation between triage code and time until the ABCDE approach. A Cochran-Armitage trend test and gamma association were used to describe the relation between the frequency with which ABCDE was used and the triage code. Fisher’s exact test compared the frequency of performed ABCDE approaches between the two different triage groups (potentially unstable or not potentially unstable). A Mann-Whitney U test was used to compare not normally distributed ABCDE scores between different groups.
RESULTS
We enrolled 270 patients and the ABCDE approach was used in 69 (26%) of them. All 270 patients were included in the data analysis. For data analysis concerning the scoring of the completeness of the ABCDE approaches, 19 of the 69 (29%) ABCDE approaches were excluded due to the following reasons: two patients waived informed consent and in 17 patients the observer had more than one patient at one time so was not able to observe both. No patients were missed due to decreased level of consciousness. Based on their triage code, 206 of 270 (76%) patients were classified as potentially unstable. In these 206 patients, the ABCDE approach was used in 67 (33%) of the cases in contrast to 2 of 64 (3%) in the stable patients (p < 0.001, table 2).
With increasing acuity of patients, defined as an increase in triage code, the ABCDE approach was applied more frequently (Gamma association r = 0.779, table 3). In patients with the highest triage code (red) the ABCDE approach was used in 100% of the cases (n = 3) while in the lowest groups (green and blue) in only 0-4 %. In patients with triage code yellow the ABCDE approach was used in only 24% of the cases.
Time delay before commencing the ABCDE approach significantly decreased by an increasing triage code (table 4). In unstable patients (triage code red and orange) the primary assessment was initiated within 10 minutes in more than 75% of patients. The duration of the ABCDE approach itself was less than 10 minutes in 75% of patients, with a median time of 7 minutes.
The ABCDE approach was not performed in 139 (67%) of the (potentially) unstable patients (those with triage code red, orange and yellow grouped together). The main reasons were: 1) the patient seemed stable after a short clinical assessment (30%), 2) the reason for the ED visit suggested a stable patient (20%), 3) the patient was first seen by a medical student who was not trained in the ABCDE approach (11%) and 4) the vital signs measured by the triage nurse suggested a stable patient (10%).
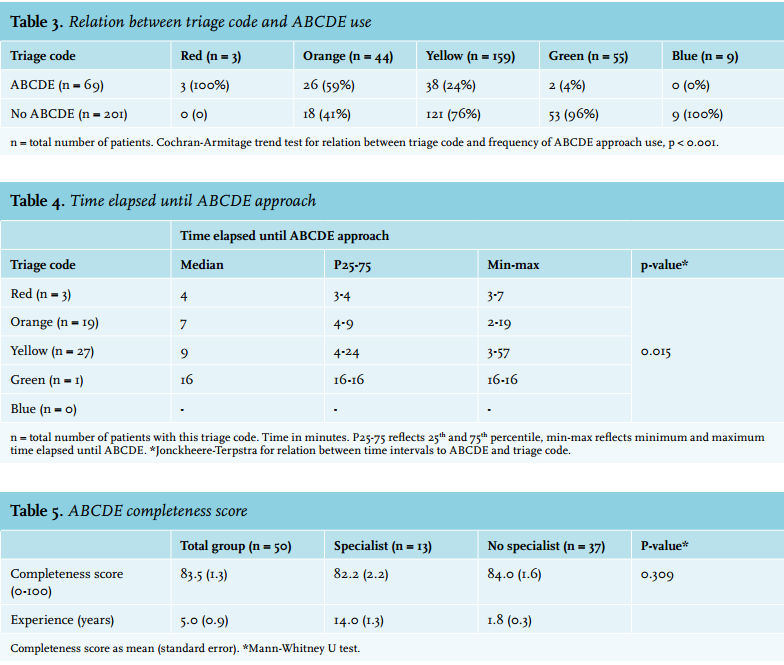
In total 50 ABCDE approaches were observed, performed by 21 different physicians including 7 consultants (grouped as specialists), 11 residents and 3 medical students (last two grouped as non-specialists) (table 5). Mean observed ABCDE approaches where 2.38 for every physician.
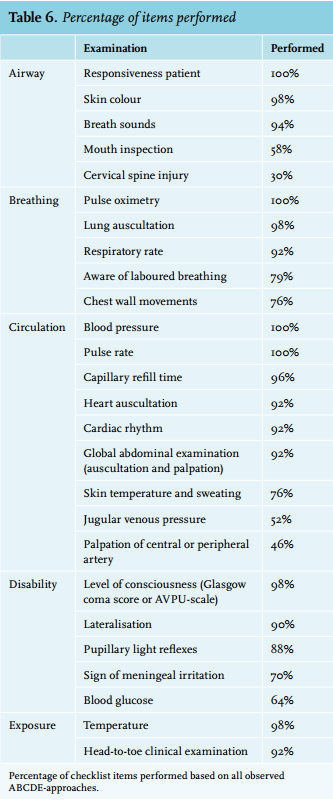
Despite the difference in years of experience between the two groups, the ABCDE completeness scores were similar (82.2 and 84.0; p = 0.309). Vital parameters were noted in every patient while investigation of cervical spine injury or palpation of central or peripheral arteries in less than 50% (table 6). 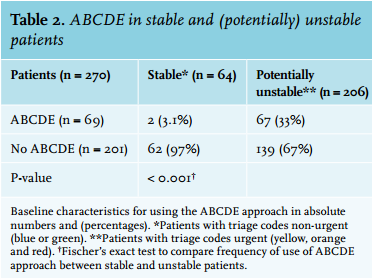
DISCUSSION
This is the first study investigating the use of the ABCDE approach in medical patients in the ED. It shows that the ABCDE approach is performed more often and sooner after admission in (potentially) unstable patients with more urgent triage codes. It was performed in 100% of patients with the highest triage code although this group included only three patients. This supports the idea that if an acutely ill patient is recognised, the ABCDE approach is the preferred method for assessing these patients. However, we found that in the majority (67%) of potentially unstable patients (those with triage code red, orange and yellow grouped together) the ABCDE approach was not used to assess the patient. In the group with the second highest triage code (orange) the ABCDE approach was performed in only 59% of patients, which decreased to 24% in patients with triage code yellow. Therefore, although the use of the ABCDE approach is associated with triage code, it is only performed in the minority of all potentially unstable patients despite the medical staff being trained to perform this approach in such patients.
We also found that if the ABCDE approach is performed, it is done efficiently with high completeness scores. There was no significant association between completeness scores and triage code. All staff and residents in our ED, except medical students, had to complete an ABCDE course before they could treat patients in the ED, which might explain the high completeness scores. Interestingly, residents and experienced staff have similar but not maximum ABCDE completeness scores (83 instead of 100) which might reflect that doctors think they do not need all the parameters to exclude potentially life-threatening diseases or stabilise the patients. For example, immediate testing for hypoglycaemia may not be necessary when the patient has a maximum Glasgow Coma Scale without signs of neurological impairment.
We tried to identify other factors, apart from triage code, affecting the use of the ABCDE approach. The main reasons for omitting the ABCDE approach were that the complete ABCDE can be performed within 10 minutes in the majority of patients, so the time benefit of performing only a clinical impressions score may not weigh up against the risk of not recognising an unstable patient. The fact that a few vital signs are normal or the medical student is not trained in treating acutely ill patients is in our opinion not a good argument to omit an ABCDE approach.
Limitations
An observational single-centre pilot study was conducted in a tertiary academic hospital. We performed a pilot study to gain insight into whether the ABCDE approach learned in a simulation-based training was applied in real practice. It is as yet unknown whether our results also apply to other EDs. We expect that in our region, the use and completeness of the ABCDE approach is lower in other EDs as we are a tertiary university hospital with multiple unstable patients presenting to our ED every day.
The physicians knew they were under observation and this may also lead to both more frequent use of the ABCDE approach and higher completeness scores in this study (the Hawthorne effect: research participants alter their behaviour when observed).10 It is possible that these scores are lower when they are not under observation and this Hawthorne effect may also partially explain the high percentage of ABCDE use in patients with the highest triage codes. Video recording is not allowed in our ED so we were not able to correct for this bias. We asked the physicians if they planned to use the ABCDE approach which may have positively influenced this number.
We only scored whether an item was performed but we did not register the quality of the ABCDE parameters or the following interventions and treatments. Although we conclude that junior doctors and staff have similar completeness scores it is possible that the actions and diagnosis after the ABCDE approach are different. In this study, it is possible that associations are not significant because of the small sample size. The checklist was developed and used by a single researcher. The Emergency Severity Index score is the triage system used in our hospital. We have chosen to group triage codes of red, orange and yellow together as potentially unstable. This might overestimate the number of patients who are labelled as potentially unstable but we believe this is the most practical cut-off value to screen for those in whom an ABCDE approach might be beneficial (high sensitivity). This study was not designed to register the clinical course of the patients in whom an ABCDE approach was omitted, so no conclusion can be made if the lack of an ABCDE approach negatively influenced patient outcome. It is currently not known if using the ABCDE approach improves patient care compared with only clinical judgment and experience. In many EDs in the Netherlands though, the treating physicians are young and inexperienced, especially during evenings and weekends. We hypothesise that the ABCDE approach might help them to improve recognition of life-threatening disease and early resuscitation. It is also not known if the potential benefits of the ABCDE approach are explained by more coordinated and intensified care or by the specific interventions itself. These are important issues to address in subsequent studies.
CONCLUSION
Our study shows that although the ABCDE primary assessment is performed more often and sooner in (potentially) unstable patients with more urgent triage codes, it was still not used in the majority (67%) of potentially unstable patients. When the ABCDE approach was used, it was performed efficiently (e.g. high completeness scores). The ABCDE approach is the preferred method, as stated by the government and several professional specialty organisations, for assessing an acutely ill patient but it seems not to be clear when to use it. Important factors determining not to use the ABCDE approach were: 1) using a short clinical impression of the patient instead, 2) stable vital signs recorded by the nurse, 3) the reason for visiting the ED suggests a stable patient and 4) the patient was first seen by a medical student who was not trained in the ABCDE approach. Currently it is not known if replacing the ABCDE approach by a short clinical impression (including only looking at a few vital signs recorded by the nurse) is a safe strategy to select patients in need for early resuscitation. Hospitals (and ABCDE courses) therefore should not only focus on teaching the content of the ABCDE itself, but also on the implementation of its use in every potentially unstable patient. More research is needed to determine whether performing the ABCDE approach indeed improves patient outcomes, since early treatment in various conditions begins with early recognition.
DISCLOSURES
The authors declare that they have no competing interests and that they have full control of all primary data. The authors agree to allow the journal to review their data if requested.
REFERENCES