KEYWORDS
Direct oral anticoagulants, patient preference, vitamin K antagonists, venous thromboembolism
INTRODUCTION
Oral anticoagulants are indicated for the prevention of stroke and systemic emboli in patients with atrial fibrillation (AF) or mechanical heart valves, and for the treatment and prevention of venous thromboembolism (VTE). For six decades vitamin K antagonists (VKA) were the only available oral anticoagulants.1,2 Although highly effective, VKA treatment has certain disadvantages, including the need for frequent INR monitoring and dose adjustments, a risk of bleeding and interactions with food and other drugs.3,4
Direct oral anticoagulants (DOACs) have been introduced as an effective and safe alternative for VKA treatment.5,6 DOACs offer a simplification of anticoagulant treatment due to their stable pharmacokinetic and pharmacodynamic profile, allowing for a fixed dose regimen. Furthermore, they are associated with a significant reduction in major bleeding events.6 Currently, four DOACs have been registered for the indications AF and VTE: the direct thrombin inhibitor dabigatran etexilate (hereafter dabigatran), and the direct factor Xa inhibitors rivaroxaban, apixaban and edoxaban.
In clinical practice, patients should be informed by their physician about both anticoagulant treatment options and their advantages and disadvantages. However, the final decision of which anticoagulant to prescribe is often made by the physician, following local guidelines and reimbursement restrictions.1,7 Patient preferences are not always considered or asked for. In a previous study in AF patients,8 the patient preferences about VKA and DOACs were investigated using a standardised questionnaire. In total 70% of patients would prefer a DOAC over a VKA when they were confronted with different scenarios highlighting the advantages of DOACs. The lack of need for laboratory control and, to a lesser extent, the lower risk of bleeding were considered the most important arguments for preferring DOACs by these patients.8
This study aims to investigate the preference of patients with a history of VTE for DOACs versus VKA using the same questionnaire. Furthermore, we explored possible predictors of treatment preference such as age, gender, treatment duration, and treatment satisfaction.
MATERIALS AND METHODS
Study population
A random sample of 200 patients was obtained from patients treated with VKA for deep vein thrombosis (DVT) or pulmonary embolism (PE) at the Thrombosis Service of Amsterdam, the Netherlands. To enrich the sample with respect to experience with VKA at the Thrombosis Service, only patients who were treated for a minimum duration of two years were considered. Hence, the following inclusion criteria were used: 1) Treatment with any VKA, 2) Treatment duration of minimally two years, 3) Treatment indication DVT and/or PE. The survey was sent to the patients by post, together with a return envelope and a recommendation letter from the director of the Thrombosis Service. All patients received a reminder three weeks after the first survey.
Survey
Patient preference for DOACs relative to VKA was assessed using a treatment trade-off technique that was administered as a questionnaire. The treatment trade-off technique allows for a comparison of patients’ therapy preference between two different treatment options.9 The current trade-off consisted of four consecutive scenarios as was the case with the previous investigation in AF patients receiving VKA.8 In each scenario, one advantage of DOAC treatment was added to the comparison. For each scenario, the patient was asked to express their preference for treatment: stay on the current VKA treatment or switch to DOAC treatment.
In scenario 1, VKA and DOACs have the same efficacy and safety. The only difference between the two options is that there is no need for laboratory control with DOAC treatment. Scenario 1 is the baseline scenario. In scenario 2, a reduced risk of major bleeding with DOAC treatment is added. Scenario 3 adds the advantage of no interactions with food and other drugs. In scenario 4, it is stated that DOACs are more effective than VKA in prevention of recurrent venous thromboembolism (VTE). Patients could indicate for each scenario whether they would definitely or probably stay with their current VKA treatment, were neutral, or would definitely or probably change to a DOAC, on a scale from 1 to 5, respectively.
Statistical analysis
The target response rate of the survey was set at 70%, with a minimum of 50%. The data on treatment preference were analysed using the generalised estimating equations (GEE) method, with a logit link, binomial distribution and an unstructured correlation. GEE enables analysis of repeated measurements or other correlated observations (such as repeatedly assessed preference). It corrects for the fact that patients’ answers to each subsequent scenario are related to their answers in previous scenarios. Outcome measures of the GEE were odds ratios and 95% confidence intervals. We calculated 1) whether there was a significant difference in the proportion of patients preferring DOAC over the four scenarios and 2) whether any of the investigated variables were significant predictors for DOAC preference.
To prepare the data for analysis, the ‘preference for DOAC’ outcome variable was dichotomised. A preference for DOACs was assigned a score of 1, and a neutral preference or preference for VKA was assigned a score of 0. Furthermore, the variable ‘educational level’ was dichotomised into ‘higher education’, including university, higher professional education, and preparatory scientific education, and ‘lower education’, including all other forms of education. The variable ‘patient age’ was analysed as a continuous variable and as a dichotomised variable separated by the sample median age. The variable ‘treatment duration’ was categorised into short VKA treatment duration (< 6 years), intermediate treatment duration (6-10 years) and long treatment duration (> 10 years) groups.
First, we evaluated the change in the percentage of patients that would switch to DOACs over the four scenarios. Second, we investigated whether several variables, such as age, gender, treatment duration, type of VKA, educational level and treatment satisfaction were associated with a preference for DOACs using the GEE method. If a variable turned out to have a significant influence on DOAC preference, the Chi-square test was used to evaluate differences between the variables’ categories for each scenario. The significance level was set at p < 0.05.
RESULTS
Response and study population
The random sample of 200 patients treated with VKA for the indication of DVT or PE who received the survey by post had a mean age of 71 years, 47% were male, and the mean VKA treatment duration was 18 years. The survey was initially sent on 16 June 2015 and a reminder was sent three weeks later.
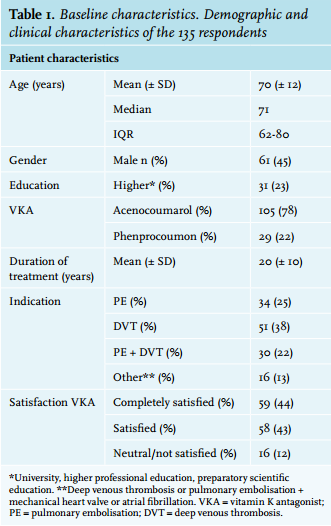
In total, 136 of those 200 patients responded with a completed survey, hence a response rate of 68%. One patient was excluded because of current rivaroxaban use, leaving 135 patients treated with VKA for inclusion in the present analysis (figure 1). Baseline characteristics of the study population are shown in table 1. The average age was 70 years (SD ± 12) and 45% of the respondents were male. The mean treatment duration was 20 years (SD ± 10), and 25% of the respondents were treated for a previous PE, 38% for a past DVT, 22% for both and 13% for previous PE or DVT with an additional indication (i.e. mechanical heart valve, atrial fibrillation). Almost 87% of the patients were (completely) satisfied with their current VKA treatment. There were missing data for three of the investigated variables. Data on type of VKA were missing in one patient, data on indication for VKA treatment were missing in four patients and data on treatment satisfaction were missing in two patients (figure 1).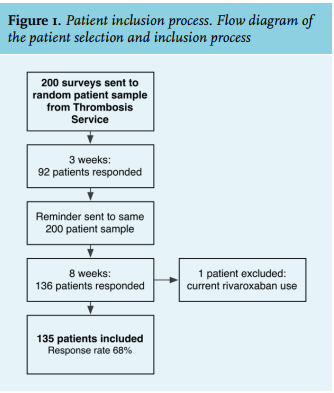
Preference for DOACs versus VKA
Figure 2 depicts the percentage of patients who would switch from their current VKA treatment to a DOAC per scenario. In scenario 1, where it is explained that DOAC treatment does not require regular laboratory controls, 36% of all patients would switch to a DOAC. In scenario 2, highlighting decreased bleeding risk with DOACs, this percentage rises to 57% (OR 2.3; 95% CI 1.6-3.3; p < 0.01). Scenario 3 added the benefit of no interactions with food or other drugs, resulting in 64% of patients preferring a DOAC (OR 3.2; 95% CI 2.2-4.6; p < 0.01 compared with scenario 1; and OR 1.4; 95% CI 1.1-1.7; p = 0.01 compared with scenario 2). The advantage of greater efficacy did not result in relevant changes in the percentages of patients who would switch to a DOAC (66%, with an OR of 3.4; 95% CI 2.4-4.8; p < 0.01 compared with scenario 1; and OR 1.1; 95% CI 0.89.1-1.3; p = 0.48 compared with scenario 3).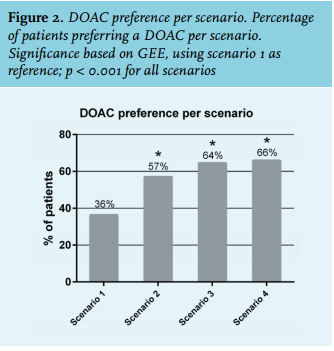
Predictors for DOAC preference
The factors gender, treatment duration, and the type of VKA (acenocoumarol or phenprocoumon) were not significantly associated with DOAC preference. In contrast, the variables treatment satisfaction, patient age, and patient education level did influence patients’ preference significantly. Data on age and treatment satisfaction were missing for two patients, whereas patient educational level was known for all patients.
Figures 3 to 5 show DOAC preference percentages for the three variables significantly associated. With regard to treatment satisfaction (figure 3), the percentage of patients switching to a DOAC rises in each consecutive scenario for all three categories of treatment satisfaction. The largest increase in DOAC preference is seen in scenario 1 to 3, mainly in the ‘neutral/not satisfied’ group. This corresponds to the trend seen in the total patient sample. However, 69% of patients who were neutral or not satisfied with their current treatment already switched to a DOAC in scenario 1, compared with 29% of patients who were completely satisfied with VKA treatment. Furthermore, of the neutral/not satisfied patients 94% preferred to switch in scenario 3, versus 53% of the completely satisfied patients.
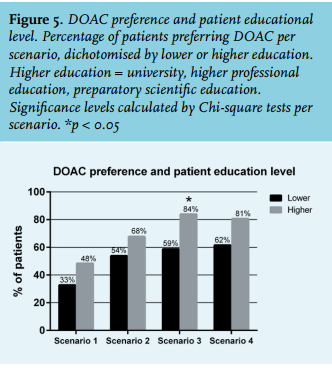
The distribution of switchers to DOAC according to age is depicted in figure 4. Again, in each consecutive scenario the percentage of patients who would switch to a DOAC increases. Patients younger than 71 years were significantly more likely to prefer DOACs in scenario 2 and 3 than their older counterparts.
Patients who had a higher education were more likely to switch to DOACs in each of the scenarios compared with patients who had received a lower education. This difference becomes significant for scenario 3 (figure 5).
When treatment satisfaction, age and educational level were combined in the analysis using the GEE, only patient age (OR 0.94 per year; 95% CI 0.94-0.997) and complete treatment satisfaction (OR 0.24; 95% CI 0.08-0.79) remained significant. For higher patient education level, the OR for DOAC preference was 1.76 (95% CI 0.85-3.64).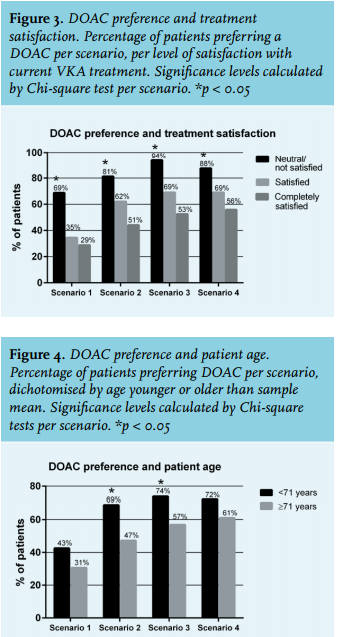
DISCUSSION
Overall, almost two-thirds of the patients in this study would prefer a DOAC over treatment with a VKA when confronted with different scenarios highlighting the advantages of DOACs. Patients considered the elimination of regular laboratory monitoring, the lower bleeding risk and the reduced interaction with food and other drugs as the most important arguments to switch to a DOAC. Efficacy on the other hand, often considered one of the most important facts by physicians, appeared to be less relevant to patients. Patient gender, treatment duration, and type of VKA were not significantly associated with DOAC preference. However, patient age, educational level, and satisfaction with VKA treatment were. Younger and higher educated patients were more likely to prefer DOACs over VKA, especially in scenarios 2 and 3, where the elements of less bleeding risk and no interaction with food or drugs were evaluated. Patients who were neutral or unsatisfied with their current treatment were significantly more likely to choose DOACs over VKA in all scenarios. Even in patients completely satisfied with VKA treatment, 51% would still like to switch to a DOAC based on the combination of a treatment simplification and a decreased bleeding risk.
As mentioned before, a comparable study using the same questionnaire was performed in patients with AF.8 There are some differences in baseline characteristics between the present study and the one in AF patients. In the current study, we included relatively more females (55% versus 43%), less patients that were highly educated (23% versus 38%), patients with a longer VKA treatment duration (20 versus 5 years) and more patients who were satisfied with their current VKA treatment (87% versus 76%). In both studies, the total percentage of patients that would switch to a DOAC is consistent at two-thirds. However, in the AF study, the lack of the need for regular laboratory monitoring and the combination hereof with reduced bleeding risk were the main arguments for switching with percentages of 57% and 65% respectively, whereas in our study the diminished interaction with food and drugs turned out to play a role as well. Another difference is that in the AF study only treatment satisfaction was found to be associated with DOAC preference,8 whereas here we observe that next to treatment satisfaction, also age and educational level played a significant role in switching to DOACs.
A strength of the current study is the high response rate of 68%. This was partly due to the return envelope provided, the accompanying recommendation letter by the director of the Thrombosis Service Amsterdam, and the reminder sent three weeks after the initial survey. Another relevant point is that the patients were randomly sampled. Therefore, our patient group is likely to be representative for VTE patients, albeit treated for a more extensive period of time.
Some aspects of this study require further comment. First, in order to enrich the sample with respect to experience with VKA treatment and the Thrombosis Service and to be able to make a comparison to the previous AF study,8 we included patients treated for at least two years. This resulted in an average treatment duration of 20 years, with some patients even treated for over 40 years. This is relatively long as most patients with DVT or PE are treated for 3-24 months after a first episode of VTE, and longer if recurrence occurs.1,10 The consequence of this selection bias is that our study is representative for patients with recurrent VTE rather than for patients with a first event. However, the results may reassure physicians that even if patients are treated for a prolonged period of time and are satisfied with their current treatment, they are open for other treatment options and willing to switch to a DOAC. Because, when presented with the advantages of DOACs, 56% of completely satisfied patients had a preference for a DOAC. The long average treatment duration could be an explanatory factor for the relatively high percentage of patients satisfied with their VKA treatment, as patients would have otherwise stopped or switched to another drug already.
Finally, the questionnaire itself has a few shortcomings. First of all, the lack of a specific antidote for DOACs at the time of study conduction was not mentioned in the questionnaire. It is at present speculation whether the lack of a reversal agent for DOACs would have led to different results. However, an antidote for dabigatran is currently available,11 and an antidote for Xa inhibitors is expected within 1-2 years.12 Second, the order in which DOAC benefits were presented in the questionnaire was the same for all patients and the scenarios were cumulative. The chosen order was the same as in the previous AF study.8 However, we do not know whether it might have influenced patients’ preference patterns. Perhaps efficacy did not add to the preference choice because it was always the last scenario presented and was in addition to the other three scenarios. Third, the trade-off technique might have been too complex for patients with a lower educational level. This might have played a role in the higher likelihood of more educated patients to choose a DOAC. Unfortunately, we cannot correct for this influence. Fourth and last, the argument added in scenario 4 is not proven to be true. Rather than more effective, DOACs are proven to be as effective as VKA. Since the drug efficacy turned out to have the least influence on patients’ preference out of all other arguments, we do not expect this has influenced our results.
Extensive trials have been completed for safety and efficacy of DOACs, but limited research has been done on the practical and subjective experiences of its users and factors influencing the treatment decision process. Further research could focus on acquiring more insight into patients’ arguments for switching or not switching to DOAC, for instance by changing the order of the scenarios. Furthermore, patients could be included in a follow-up, to retrospectively investigate factors influencing treatment preference in patients who ultimately did or did not switch to DOAC treatment.
In conclusion, almost two-thirds of patients had a preference for DOACs. Patients considered the lack of need for regular laboratory monitoring, the lower risk of serious bleeding and the absence of interactions with food and other drugs the most important arguments for switching to a DOAC. Efficacy was considered less important. Patients who were less satisfied with their current treatment, younger patients and patients with higher education were more likely to prefer a DOAC over a VKA.
ACKNOWLEDGEMENT
We would like to thank all patients who participated in this study.
DISCLOSURES
This study did not receive any financial support.
The following conflicts of interest apply: M.P.A. Brekelmans, M. Kappelhof and P.T. Nieuwkerk report no conflict of interest for this study. M. Nierman is the current director of the Thrombosis Service Amsterdam (Atalmedial). H.R. Buller has served as a consultant to Sanofi-Aventis, Bayer, Pfizer, Glaxo-Smith-Kline, Astellas, Boehringer-Ingelheim and Daiichi-Sankyo, outside of the submitted work. M. Coppens has received consultancy and lecturing fees, as well as research support from Daiichi-Sankyo, Boehringer-Ingelheim, Bayer, Bristol Myers-Squibb, Pfizer and Sanquin Blood Supply, outside of the submitted work.
REFERENCES