As emergency departments (ED) around the world evolve their protocols in adapting to an ageing society with potentially complex biomedical and psychosocial stressors overlying acute illness or injury, feasible and adequately accurate risk stratification for ‘vulnerability’ will become a cornerstone of older patient’s care in the ED. Although multiple ED instruments exist for this purpose, none accurately identifies either high-risk or low-risk older adults.1 Ideally, an instrument suitable for the ED risk stratification of complex older adults would accurately and reliably identify both high- and low-risk individuals across a variety of illness and injury presentations for heterogeneous populations, without requiring any extra equipment, personnel, or time to which every hospital has access.2
De Gelder et al. report the derivation and validation of a prediction model for the composite outcome of functional decline and mortality at 90 days following an ED visit for 1632 non-critically ill patients over the age of 70, excluding acute myocardial infarction or stroke patients who were eligible for thrombolysis.3 Approximately one in three suffered functional decline or death and the authors report a six-item predictive model that includes age, ambulance arrival, number of medications, assistance required for bathing or showering, prior hospital admission in the preceding six months, and history of dementia. The prognostic accuracy of this new model to identify patients at increased risk for these post-ED adverse outcomes compared favourably with the Identification of Seniors at Risk (ISAR), particularly for the highest-risk patients. The Acutely Presenting Older Patient (APOP) study is another important piece of the puzzle as clinicians and epidemiologists merge efforts to understand, measure, and interpret the components of vulnerability identified during an ED visit, but the work must continue.
Deriving, validating, and implementing clinical prediction instruments represents a long-term endeavour fraught with frequent dead-ends. Multiple examples exist of promising tools for ED scenarios such as transient ischaemic attack, myocardial infarction, and geriatric vulnerability that subsequently failed to be sufficiently accurate when applied in different settings.4 The unique challenges for building these instruments to assess ‘vulnerability’ in the fast-paced ED environment and for complex older adults have been well described and are summarised in table 1.1,2 Key decisions surrounding the process of using these instruments include a focus on screening (widespread assessment of high- and non-high-risk individuals) or case-finding (targeting at risk individuals), as well as designing for implementation by ensuring that the instrument can be interpreted and administered by diverse individuals in the ED (volunteers, technicians, nurses, physicians). Assessing the quality of these instruments includes contemplation about the primary objective to identify increased risk (high likelihood ratio) or decreased risk (low likelihood ratio) subsets, since decision instruments generally cannot do both. Closely related to this objective-defining decision is understanding how accurate ‘good enough’ is to support widespread adoption of the instrument into guidelines and routine clinical practice? The rule of thumb for a positive or negative likelihood ratio is greater than 10 or less than 0.1, respectively, but none of the existing instruments attain this level of accuracy (yet).5 While clinicians await more accurate instruments, how will key stakeholders’ perspectives and interpretation of risk stratification be evaluated? For example, if geriatricians, primary care providers, trauma surgeons, or orthopaedic specialists fail to accept the validity of these instruments then it is unlikely that ED provider’s disposition and management recommendations that incorporate the risk assessment will be valued. These stakeholders also include patients and families, as well as governmental insurers who set policy that sometimes links higher quality care to healthcare reimbursements.6
The individual components from which these instruments are derived and further validated also require standardisation across nations, languages, and healthcare landscapes. For example, De Gelder et al. use the Six Item Cognitive Impairment test to define dementia, but reference a non-ED study as proof-of-concept for the face validity of this instrument. In fact, one ED-based study of this instrument indicated that it accurately identifies patients at low risk for non-delirium cognitive impairment, but does not identify high-risk individuals so one could argue whether patients were correctly analysed as to the presence or absence of dementia in the current study.7
Reviewing studies from Australia, Asia, Europe, and North America, clinicians will find a large variety of instruments employed to measure geriatric syndromes such as dementia, delirium, comorbid illness burden, and illness acuity which represents a veritable Tower of Babel for those trying to compare one population, instrument, or intervention against another. Additionally, under-utilised qualifiers for global dysfunction such as frailty exist,8,9 as well as descriptors of outcomes as ‘preventable ED returns’.1 As more researchers derive and evaluate new instruments against previous models, investigators and funders must agree upon a package of measures that are mutually acceptable in order for others to compare one study’s results to another.
Even if key process, quality, and definitional issues are addressed, a largely unanswered question is what to do with the added information from ED vulnerability assessments? At a threshold of ≥ 2 the ISAR identifies 61% of individuals as high risk, while the APOP composite outcome instrument identified over 25% of individuals as amongst the 30% highest risk. Should all of these individuals be admitted to the hospital? If not, which subset can be safely managed as outpatients? Does a one-size-fits-all intervention exist to reduce short-term adverse outcomes or is an individualised approach required? If individualised interventions are needed, which is most likely, then how (and by whom) would this additional assessment occur?
Assessing older adult’s vulnerability for short-term adverse outcomes following an episode of ED care is recommended by educators10 and professional guidelines,11,12 but clinician’s ability to accurately do so remains elusive. In addition to the APOP investigators, ED researchers worldwide are exploring different approaches to distinguish older adults at increased risk for preventable suboptimal outcomes.13-15 Opportunity exists concurrently with abundant challenges, but assessing ED elder’s vulnerability provides the prospect for multidisciplinary, international investigators to collaboratively align emergency care with patient-centric priorities that improves the efficiency and quality of healthcare delivery. Progress awaits these ongoing efforts and will require persistent and substantial energy, funding, and innovation.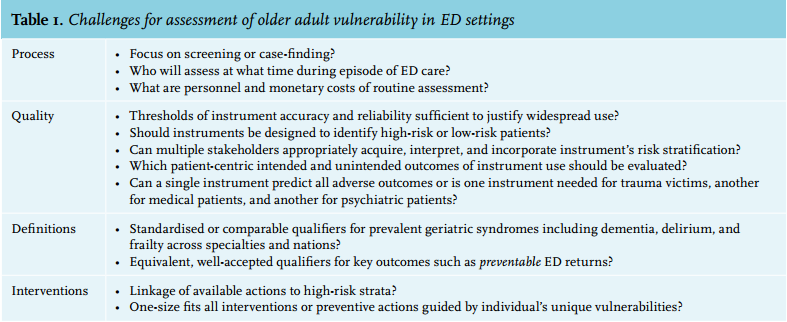
REFERENCES