KEYWORDS
Treatment preferences, decision-making, willingness to pay, chemotherapy, costs-valuation
INTRODUCTION
While chemotherapy for the treatment of cancer is expected to bring an overall benefit, it may also be associated with significant side effects. An optimal treatment is an individual decision which may result from the interaction between physician and patient. Many patients prefer and endorse shared decision-making with their physician.1,2 During decision-making both parties should carefully weigh the relative harms and benefits of chemotherapy.
Understanding treatment preferences is essential for optimal decision-making. While some patients try intensive treatments that are unlikely to help, others avoid mild treatments that may cure.3 The healthcare professionals’ view on the impact of treatment on patients’ quality of life may differ from the patients’ view in this respect. Therefore, it is important to obtain insight into both patients’ and physicians’ attitudes towards chemotherapy.
Various strategies are available to assess preferences for cancer treatments.4 A pivotal British study assessed attitudes to chemotherapy by designing hypothetical scenarios with intensive and mild treatment regimens.5
Participants were asked to rate the minimal benefit to make therapy worthwhile in terms of possibility of cure, survival gain and symptom relief. Several studies based their questionnaire on this classic method. Bremnes et al. repeated a comparable study in Scandinavia and in a study by Extermann et al. differences in preferences between French and American cancer patients were determined.6,7
A review of international published literature showed that the treatment benefit that patients desire is small; however, the variance in preferences within studies is large.8
Little is known about preferences for cancer treatment in the Netherlands. In the past two decades, a few Dutch studies were performed examining treatment preferences and decision-making.9-12 Most of these studies focused on specific cancer types in a curative/adjuvant setting. For example, Jansen et al. examined preferences for adjuvant chemotherapy in early-stage breast cancer.10
Breast cancer patients, who were about to start with and without chemotherapy, were asked to indicate the minimal benefit to make adjuvant chemotherapy acceptable. Patients with chemotherapy accepted therapy for significantly less benefit than their counterparts without chemotherapy. Generally, most of these Dutch studies focused on specific cancer types in a curative/adjuvant setting.
The negative aspects of anticancer therapy are not limited to the physical side effects for individual patients, but also include the costs of therapy. Costs of cancer care are high and expected to rise worldwide, thereby forcing decisions by healthcare policy makers. The annual costs for cancer care in the Netherlands have increased from €3.4 billion in 2007 to €4.8 billion in 2011, of which 9.8% was spent on drugs.13 This upward trend is a result of factors such as the introduction of new medical technology for specific individual cancer treatment, the development of new anticancer therapies, the extension of cancer care and the ageing population.14 In the majority of cost-analysing studies participants are asked to bid for a treatment by using bidding game strategies.15,16 However, in countries with an advanced integrated healthcare system, the personal financial contribution is minimal. Therefore, it is more interesting to focus on public opinion towards capacity of insurances and the societal costs in cancer care.
The aim of this study was to determine cancer patients’, non-cancer patients’ and healthcare professionals’ desired minimal benefits to make a chemotherapy-based treatment worthwhile, and to examine the degree of involvement during decision-making. A secondary objective was to assess attitudes towards cancer costs. In this article we report the data of a written survey that was performed among patients, with and without cancer, and healthcare professionals in the Netherlands.
METHODS
Design
The study design was a multisite prospective survey, performed by the Radboud University Medical Centre (Radboudumc) Nijmegen in collaboration with the teaching hospital Medisch Spectrum Twente (MST) Enschede, the Netherlands. The survey was performed between June and November 2013.
Questionnaire
The questionnaire assessed three main areas: questions directed to (1) treatment preferences and decision-making, (2) attitudes towards costs of cancer therapies and (3) information on demographics and the type of malignancy. Implementation of the survey was completely anonymous. When conducting this study no identifying information was collected from the participants.
Questions about preferences for chemotherapy were comparable with the original format designed by Slevin et al.5 The original questions were translated into Dutch. In order to make the questionnaire easy to read we modified the layout into visual attributes. Two hypothetical chemotherapy-based scenarios were described along with their risks and side effects: an intensive toxic and mild regimen respectively. The intensive regimen described chemotherapy with a high risk of side effects and a higher risk of infections, bleeding complications and hospitalisation. The mild regimen described a chemotherapy schedule with less risk and side effects. Subjects were asked to rate their desired minimal benefit to make therapy acceptable in terms of probability of cure, life prolongation and cancer symptom relief. Alternatives ranged from 0 to 100% and from 0 to 60 months, respectively.
Attitudes towards cancer costs (not restricted to chemotherapy) were examined using willingness to pay-like questions. As it is not common for Dutch people to pay out-of-pocket for healthcare, we used a simplified payment scale of Mitchell and Carson.17,18 Participants were asked to indicate the maximum cost – covered by healthcare insurance – for a novel treatment that only prolongs survival by an extra three months. This question was incorporated into two hypothetical patient-based scenarios, one describing a cancer patient with a poor performance state and another describing a patient with a good performance. Costs were arranged from €2000 to more than €50,000 per month.
The last area focused on demographic factors including age, sex, education level, race or ethnic group, marital status and gross annual household income. Participants’ preferred involvement in decision-making was determined using a translated Control Preferences Scale (CPS). The CPS is a validated and widely used scale containing five levels of participation in decision-making.19 Cancer patients were also asked about disease-specific characteristics, such as cancer type, treatment intent, presence of metastases and duration of treatment. With regard to anonymity, no additional information was searched to validate the patient’s perception about these characteristics.
According to Eurostat, the statistical office of the European Union, a new questionnaire should be tested at least once with potential respondents.20 Therefore, two pilots were carried out to test the applicability of the questionnaire. Cancer patients (n = 25) and medical students (n = 18) were asked to critically assess the questions. Ultimately, based on our observations and their comments, we redesigned our final questionnaire.
Data collection
The population of this study consisted of three main groups: (1) patients currently on treatment for cancer, (2) patients without cancer, and (3) healthcare professionals. All included subjects were 18 years and older, and had a sufficient understanding of the Dutch language.
Between June and November 2013, 163 cancer patients who attended the Radboudumc and MST for outpatient chemotherapy or targeted therapy were asked to complete the questionnaire. Cancer patients who received hormonal therapy only were excluded. A total of 101 subjects without cancer were approached at the department of endocrinology (MST) and at the department of orthopaedics (Radboudumc). Patients were informed in person about the study intent, and were then asked to participate. To avoid external influences, participants were asked to complete the questionnaire individually.
In the same period, 400 healthcare professionals (physicians, primary care physicians and nurses), currently working in healthcare, received the questionnaire with an envelope for return and a link for online answering. The group of professionals consisted of either oncological or non-oncological medical specialists and nurses from both hospitals.
The response rate among cancer and non-cancer patients was 90.2% (n = 147) and 87.1% (n = 88), respectively. Among healthcare professionals, this rate was 44%, with 10.2% (n = 18) using the Internet to answer the questions. In total 35 questionnaires were excluded from data analysis because of incompleteness (n = 19) or because control patients or professionals reported a history of cancer (n = 16). Finally, 382 questionnaires (139 cancer, 82 non-cancer and 161 healthcare professionals, respectively) were used for data analysis.
Data analyses
All data were collected on standardised forms and statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) software (version 20.0.0.1, IBM Corporation).
Continuous variables were displayed with an average (mean) and standard deviation (SD) or, in case of a non-normal distribution, as median and range. The normality was assessed by visual interpretation of histograms. Categorical variables were displayed as frequency (n) and percentage (%).
Differences between categorical variables in participant demographics were calculated by using chi-squared tests. Differences between continuous variables were calculated by using the unpaired T-test (with Welch correction if applicable) and, if data were not sampled from a Gaussian distribution, a non-parametric test was performed.
The relation between participants’ characteristics, treatment preferences and indicated costs was determined by using Spearman’s rank correlation coefficient (age), chi-squared (χ2 ) (gender, ethnicity, marital status) and one-way analysis of variance (ANOVA) (income, education level) at univariate level. The Holm-Bonferroni method was used to counteract the problem of multiple comparisons. We constructed multivariate linear regression models to examine whether differences in treatment preferences between groups were related to the differences in demographic characteristics that were observed (variables with a p < 0.15 at univariate level). All statistical tests were two tailed. Differences were considered statistically significant at p < 0.05)
RESULTS
Participants’ characteristics
Table 1 presents the characteristics of cancer patients, non-cancer patients and healthcare professionals. Cancer patients were significantly older in comparison with non-cancer patients and healthcare professionals (mean age 61 years; SD 14.5 years, 51 years; SD 17.5 years, and 41 year; SD 11 respectively, p < 0.001). While education level and gross income differed between healthcare professionals and the two patient groups, there was no difference between cancer and non-cancer patients.
Fifty-eight percent of cancer patients (78/134) were treated with palliative intent. Of these patients, 30% (41/134) were diagnosed with cancer less than three months ago and 87/139 patients (63%) had known metastatic disease. The most common cancers in the MST were breast (33%), colorectal (20%), and haematological malignancies (22%). Because the Radboudumc is a tertiary care centre, a higher percentage of rare tumours (sarcomas, head and neck cancers) was observed (table 1). The majority of participants desired an active participation in decisions about cancer treatment (shared decision-making). Healthcare professionals (as surrogate patients) more often opted for the option 'Only I decide' or 'Especially I decide'.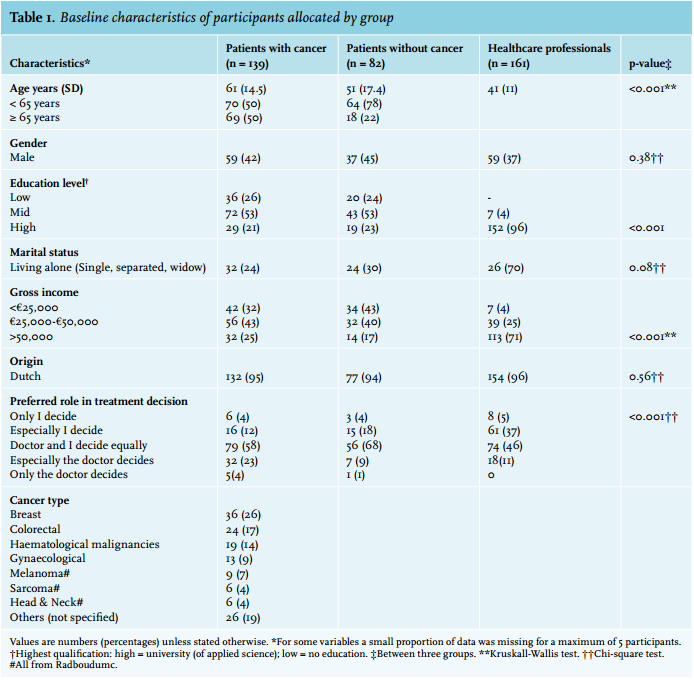
Treatment preferences
According to the two hypothetical chemotherapy regimens, subjects were first asked if ‘under any circumstances’ they would accept a mild or intensive cancer treatment (table 2a). For both regimes, the level of rejection was similar for cancer patients and non-cancer patients. Healthcare professionals were significantly more willing to accept chemotherapy compared with cancer patients and non-cancer patients (p = 0.01), with none of the professionals rejecting the mild regimen and 4.3% rejecting the intensive regime. Fifteen participants (4.5%, only patients) were willing to undergo the intensive therapy but not the mild therapy.
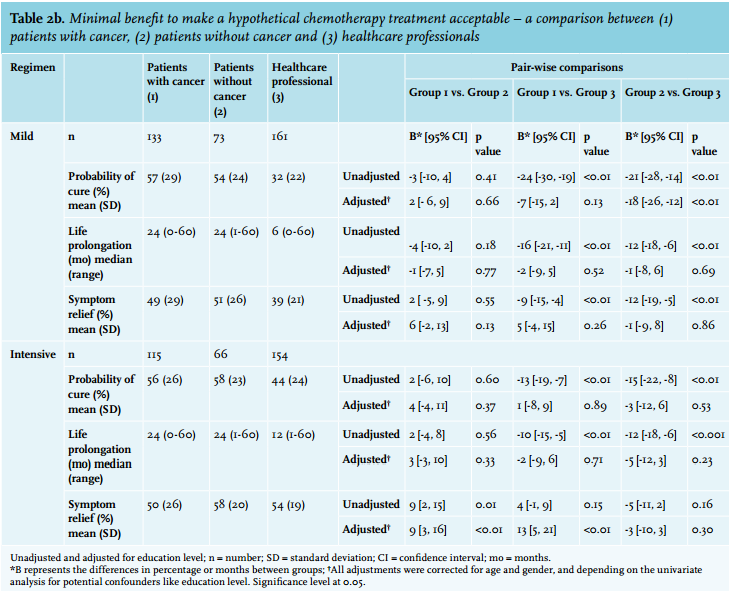
Participants who were willing to undergo a mild or an intensive regimen were asked to indicate a minimal desired treatment benefit in terms of cure, life prolongation and relief of symptoms (table 2b). Overall, the mean threshold for accepting a toxic regimen was higher or equivalent to that of the mild regimen. About 50% of all patients and 41.6% of the healthcare professionals desired the same level of cure from both regimens. Remarkably, 9.4% of all patients indicated to want a higher benefit from the mild treatment. As presented by the unadjusted analyses, healthcare professionals demanded significantly less benefits from both therapies compared with cancer and non-cancer patients. No difference was found between cancer and non-cancer patients. Sub-analyses between oncology-oriented healthcare professionals (concerning both physicians and nurses, n = 51) and non-oncology healthcare professionals (remaining healthcare professionals, n = 108) showed no significant differences in willingness to undergo chemotherapy or indicated treatment benefit for both regimens.
To examine whether differences in preferences between groups are related to the differences in the demographic characteristics that were found, we adjusted for possible confounders. At an univariate level, the variables age, education level and gross income showed associations (data not shown). The variable gross household income was not put in the multivariate model, because of its collinearity with the education level. At multivariate level only the factor education level was an important explanatory determinant; adjusted for education, the observed difference between healthcare professionals and patients was no longer significant. Highly educated subjects accepted chemotherapy for significantly less benefit (mostly p < 0.001) compared with low-educated participants (table 2b). Although the average age between the three groups is different, there was no relation between age and indicated treatment benefits at the multivariate level.
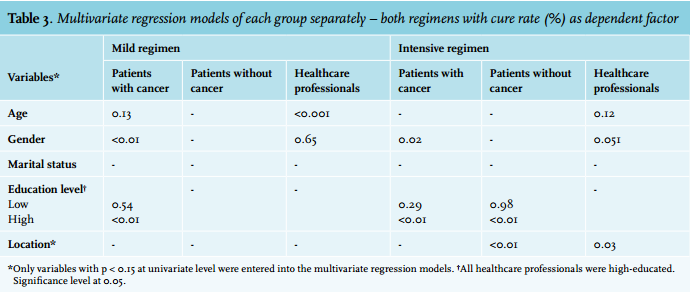
Table 3 presents the relationships between baseline characteristics and treatment preferences in each group separately. In these models, treatment benefit is expressed by the desired cure rate. In patients with cancer, education and gender were associated with the desired treatment benefit. A higher education level was associated with lower treatment benefits for both cancer patients and non-cancer patients (in case of a heavy treatment regimen). With regard to chance of cure, female cancer patients were significantly (p < 0.05 in both regimens) more reluctant to undergo a mild (p < 0.01) or intensive regimen (p = 0.02) compared with men. However, in the group of healthcare professionals, men were more reluctant compared with their female colleagues to accept an intensive regimen (p = 0.04). Among cancer patients no correlation was found between age and desired cure rate. For healthcare professionals, there was a positive correlation between age and desired cure rate in the mild regimen (p < 0.001). In the intensive treatment regimen the p value was 0.12. 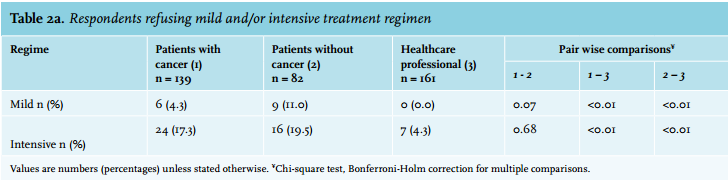
Cost valuation
Participants were presented a hypothetical situation in which they had cancer and were offered cancer treatment with a three-month survival benefit. They were asked to rate the maximum acceptable costs of this treatment. This was done for two hypothetical situations: one with a good performance state (scenario A) and one with a poor performance state (scenario B). Figure 1 shows the results per survey group. Cancer patients accepted higher costs in both scenarios compared with healthcare professionals (good performance state p = 0.018; poor performance state p = 0.012). Between cancer patients and non-cancer patients there was no difference in valuation. A remarkable number of cancer patients (n = 27; 21.6%), non-cancer patients (n = 14; 17.9%) and healthcare professionals (n = 14; 8.9%) found a cost of more than €50,000 per month acceptable.
In all groups, the maximum acceptable costs of a cancer treatment for good performance state were significantly (p < 0.001) higher than for poor performance state, despite a comparable hypothetical survival gain in both scenarios. In contrast, about 5.3% (19/357) indicated a higher amount for a hypothetical new treatment acceptable in a patient in a poor performance state. For 60.5 (216/357) of participants, performance status had no influence on the maximum acceptable costs.
Again education level was of influence (the less educated accepted higher costs). No relations were found for age, gender and marital status.
DISCUSSION
We studied the willingness to accept chemotherapy and the attitudes towards of costs of cancer treatment in the Netherlands.
The main conclusions of our study are: (1) almost all patients accept chemotherapy, although the majority indicate unrealistic goals, (2) education level has a significant influence on preferences, while age only gave different views when tested univariately, and lastly, (3) regarding costs in cancer care, many cancer and non-cancer patients opted for higher cost options, thereby indicating that cancer costs should not be a topic of discussion according to patients.
Treatment preferences
The results of this study show a significant difference between patients and healthcare professionals. While minimal benefits did not differ between cancer patients and non-cancer patients, with respect to chance of cure, life prolongation and symptom relief, healthcare professionals were likely to accept chemotherapy for lower thresholds. Education level was the most important explanatory variable. Remarkably, the differences between patients and healthcare professionals disappeared when correction for education level was applied.
Despite a wide variety in desired benefit, the average desired benefit of both cancer and non-cancer patients accepting chemotherapy was high and beyond what is realistically achievable in most settings. This finding is contrary to the observed thresholds by Slevin et al.5 However, two smaller but methodologically comparable studies by Bremnes6 and Extermann7 reported findings comparable to our study.
Given the indicated desired benefit, patients have too high expectations of chemotherapy. These unrealistic expectations are consistent with other studies demonstrating discordance between unrealistic expectations of patients and physicians’ beliefs about treatment.21,22 While high expectations of non-cancer patients could be explained by lack of familiarity with the treatment effect expected, all cancer patients in this study received chemotherapy with generally presumed less benefit compared with their indicated preferences in the given hypothetical situation. There are several explanations for these unrealistic expectations. A Dutch cancer-specific ethnographic study described that collusion between the cancer patient and physician (with explicit focusing on chemotherapy effects) may facilitate unrealistic optimism and unjustified hope.23 ‘Not giving up’ is an attitude for physician and patient to reinforce considerations about chemotherapy.24 Other factors include inability of physicians to communicate adequately about expected prognosis and using complex terminology, which is sometimes too difficult for patients to understand.23,25
Because the majority of participants indicated to prefer ‘shared decision-making’, the discrepancy in treatment preferences between patients and healthcare professionals emphasise the importance of carefully discussing preferences and expectations before starting treatment.
Level of education appeared the most important extensive explanatory variable. An explanation for this finding could be that higher educated people have more knowledge about chemotherapy and therefore assess the risk/benefit ratio differently. Surprisingly, age did not appear to be of influence in the two patient groups. In contrast to previous studies, there was no difference in desired benefit between younger and senior patients (70 years and older).10,26 As a result of the growing participation of the elderly in education with a better financial, health and care situation, older patients are more self-conscious and therefore perhaps more willing to undergo treatment.27 As a consequence of this emancipation, age no longer seems to be a limiting factor.
Attitudes towards cancer costs
Recently, the costs of cancer care generated widespread headlines, and the Dutch Cancer Society wrote a report on accessibility of cancer drugs.27 However, patients’ preferences concerning costs of cancer treatment are relatively unknown. The annual Dutch costs of new anticancer agents are approximately €60,000 to 80,000 per patient. Most of these new agents do not cure, but only prolong life. Attitudes towards cancer costs varied between the three groups, with healthcare professionals accepting significantly lower maximum cost options in comparison with cancer patients. As expected, participants accepted higher costs for a patient with a good performance state. Many patients and non-cancer patients opted for the highest possible answer option ‘€50,000 or more per month’, thereby indicating that cancer costs should not be a topic of discussion. Because costs of cancer care are directly covered by healthcare insurance in the Netherlands, most patients are unaware of the actual costs of their treatment and do not discuss treatment costs with their physician. This unawareness makes it hard to realise the personal economic burden of treatment costs. Although in this study participants were not directly asked on their view on the treatment cost debate, the questions about cost gave rise to emotional feedback, in which most patients emphasised that treatment costs should not influence the treatment and not be discussed directly between doctor and patient. Focusing on healthcare professionals, most professionals opted for low cost options (€2000 to €5000 per month). However, a small percentage indicated the highest possible amount. This finding emphasises a mismatch between one of the CanMEDS1 competencies: ‘The responsible use of healthcare recourses’ and the individual physician who wants the best for his patient, regardless the costs. To gain more insight into attitudes towards cancer costs, new methodologies need to be developed, so that study results can be better compared and be uniform.28 Physicians and policy makers will thus gain more insight into the value of health.
Lower educated participants with lower incomes indicated significantly higher values for treatment costs. This finding is contrary to several willingness to pay studies where income was related to the willingness to pay.16,29,30 A possible explanation for this finding lies in the extension of the earlier mentioned relation between education level and desired treatment benefits. Higher educated participants, generally having higher incomes, may be more aware that an increasing amount of the gross domestic product is spent on healthcare and that this continuing increase is not durable in the long run.
Strengths and weaknesses of the present study
The strength of the present study includes the unique concept of analysing treatment preferences and attitudes towards societal cost in the Netherlands. By including participants in different regions and two different practice settings – an academic centre (Radboudumc) and a general hospital (MST) - we have probably created a representative Dutch patient population.
However, there are several limitations to be noted. First, because all participating cancer patients received chemotherapy and therefore already discussed treatment options and preferences with their physician, it is possible that they have a more positive view regarding therapy compared with cancer patients not scheduled for chemotherapy. Besides, because this study was carried out in a hypothetical situation, cancer patient preferences may have been influenced by the effect of reconciliation with the treatment decisions they have made before.31
A second important methodological limitation is related to the use of a questionnaire. Despite intensive testing and revision of the questionnaire, a small number of participants (less than 10%) desired conflicting treatment outcomes by indicating higher treatment benefits of a mild regimen, compared with an intensive regimen, suggesting they did not interpret the questions correctly. In addition to the present study, the next step would be to assess preferences of cancer patients and physicians by investigating underlying social-economic factors and using other strategies such as discrete choice and trade-off experiments. Combining these experiments with personal interviews would be an important addition to understand these, sometimes remarkable, outcomes. Application of willingness to pay strategies to analyse costs remains difficult, especially in Western Europe, where the healthcare system is organised differently compared with other parts of the world. Within this field, patients’ perspectives regarding cancer costs are poorly studied.25 Simplified and validated methods are needed to better assess attitudes towards cancer costs.
PREVIOUSLY PUBLISHED
Poster presentation SIOG (International Society of Geriatric Oncology) 2013 congress Copenhagen Denmark on 24 to 26 October 2013. Title: ‘Preferences for treatments in medical oncology: a multisite, prospective survey study in the Netherlands’.
ACKNOWLEDGEMENTS
We are very grateful for the participation of all patients and healthcare professionals. We would like to thank all members of the department of oncology (Radboudumc and MST), orthopaedics (Radboudumc) and endocrinology (MST) for their support in approaching patients. And special thanks to E.M.M. Adang (associate professor health technology assessment) and P.F.M. Stalmeier (senior researcher health technology assessment), both from the department of Health Evidence (Radboudumc), for their assistance in statistical analysis and editing the questionnaire.
Competing Interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure. pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: This study was approved by the regional medical ethics commission CMO (Commissie Mensgebonden Onderzoek, region Arnhem-Nijmegen). Registration number: 2013/254.
REFERENCES