KEYWORDS
Diet, gestational diabetes mellitus, insulin therapy, predictors, risk stratification
INTRODUCTION
Gestational diabetes mellitus (GDM) is one of the most common metabolic complications during pregnancy and occurs in 1-14% of all pregnancies, depending on the population demographics and the diagnostic criteria used.1 Given that obesity is a worldwide epidemic and the recent more stringent guidelines for screening and diagnosis, the prevalence of GDM is still increasing which burdens obstetric care systems.2-7
GDM is associated with an elevated risk of adverse obstetric and neonatal outcomes during pregnancy.8-11 However, studies demonstrated that GDM is a treatable condition and controlling blood glucose levels throughout pregnancy can reduce the risk of complications.12,13 Dietary advice is the first step and cornerstone in GDM treatment. When diet fails, insulin therapy is the second step in treatment, according to almost all the international guidelines.14
In our country, we have a special obstetric care system which is divided between primary and secondary care. The primary care is organised by independently practising midwives and general practitioners (GPs) who take care of normal pregnancy and childbirth, and secondary care is organised by in-hospital obstetricians and specialised clinical midwives caring for pathological pregnancy and childbirth or pregnancies accompanied by comorbidity.15
Since GDM pregnancies are at increased risk for adverse obstetric and neonatal outcomes, women with GDM are referred to hospitals for obstetric care and are advised to give birth in a hospital with good neonatal facilities. This is especially applicable for women with GDM who are treated with additional insulin therapy and who are considered to represent a more severe GDM group due to a greater difficulty to maintain glycaemic control.16
However, there may be ‘low-risk’ women with GDM who do not need obstetric care in secondary care but can maintain care from their midwives or GPs. Women with GDM treated with diet only might be a potential ‘low-risk’ group who could be treated in a low-risk setting and even qualify for delivery at home. Such a policy demands the correct identification of women with GDM with a high-risk of adverse pregnancy outcomes.
In an earlier paper, we reported the neonatal and obstetric outcomes of pregnancies complicated with GDM after implementation of the 2010 Dutch Society of Obstetrics and Gynaecology GDM guideline on screening and treatment – diet only versus additional insulin therapy – and we compared these outcomes with the general obstetric population in the Northern region of the Netherlands.17 In the present study we aim to identify relevant factors predicting the need for insulin therapy in women with GDM and secondly to determine a potential ‘low-risk’ diet-treated group likely to have good obstetric and/or neonatal outcomes.
MATERIALS AND METHODS
Study population and design
The study population consisted of all women with singleton pregnancies who were diagnosed with GDM according to the Dutch national guidelines in the University Medical Center Groningen and in the Martini Hospital Groningen, between January 2011 and September 2014. As previously reported,17 pregnant women were recommended to undergo a 75-gram oral glucose tolerance test (OGTT) at week 24-28 of gestation if they had one or more risk factors for GDM according to the Dutch national guideline: previous GDM, first-degree relative with type 2 diabetes mellitus (DM), a previous neonate weighing ≥ 4500 gram, pre-pregnancy body mass index (BMI) ≥ 30 kg/m2 , some ethnic risk groups (South-Asian, Hindu, African-Caribbean, Middle Eastern, Morocco and Egypt), history of intrauterine foetal death (IUFD), and history of polycystic ovary syndrome (PCOS). Also women with signs suggestive of GDM (e.g. polyhydramnios and/ or foetal macrosomia) were screened.14 Women with previous GDM were screened at week 16-18 of gestation and when the test was negative, it was repeated at week 24-28 of gestation. GDM was diagnosed if the fasting plasma glucose was ≥ 7.0 mmol/l and/or the two-hour plasma glucose ≥ 7.8 mmol/l. In addition, GDM was diagnosed if the fasting glucose was > 7.0 mmol/l or random glucose was > 11.1 mmol/l.14,18 The guideline uses these diagnostic criteria, based on the criteria of the World Health Organization (WHO) 1999.18
Women with a twin pregnancy (n = 15) and women with missing data on neonatal complications (n = 4) were excluded. Women with pre-existing diabetes were not included in the study. This study has been exempted for approval according to the Medical Research Involving Human Subjects Act. This report is based on patient data acquired during care as usual, the data were analysed retrospectively and all the requirements for patient anonymity are in agreement with the regulations of the ethics committee of both hospitals. According to this and the Dutch law on Medical Research with Human Subjects, no approval from an ethics committee is necessary.
GDM treatment regimens
All women diagnosed with GDM received dietary advice by a trained dietician, which included education about carbohydrate intake and carbohydrate distribution. The women also received instructions regarding self-monitoring of blood glucose levels by a diabetes specialist nurse and were instructed to measure fasting and one-hour postprandial blood glucose levels every day for one week. After 1-2 weeks the blood glucoses values were evaluated at the diabetes outpatient clinic. If the fasting plasma glucose level was ≥ 5.3 mmol/l and/or postprandial plasma glucose level ≥ 7.8 mmol/l additional insulin therapy was started. Insulin was commenced with two elevated blood glucose levels on two successive days and no expected benefits of further dietary intervention. There were three options for insulin therapy: once daily long-acting, prandial ultrashort-acting insulin or a combination of both (basal-bolus regimen), depending on the specific glycaemic profile. In both centres short-acting insulin analogues and NPH insulin were used in GDM treatment.
Measures
All data were assessed from medical and birth records. Ethnicity was classified into four categories: Caucasian, African-American, Middle-Eastern/North-African descents, and Asian (Indian or South-East Asian). Family history of diabetes was defined as having a first-degree relative with type 2 DM. Weight gain was calculated from pre-pregnancy weight to the first visit. HbA1c values were measured by standardised HPLC method on a Tosoh G8 system (Tosoh, Tokyo, Japan), considering 22-42 mmol/ mol (4.2-6.0%) as normal. The HbA1c values were measured at the time of GDM diagnosis within one week after the OGTT.
Neonatal complications included: a composite outcome of perinatal complications (still-birth/neonatal death, birth trauma (shoulder dystocia, fracture of humerus or clavicle), hyperbilirubinaemia and neonatal hypoglycaemia), large for gestational age (defined as birth weight above the 90th percentile, adjusted for age, gender, parity, and ethnicity19), small for gestational age (defined as birth weight below the 10th percentile, adjusted for age, gender, parity, and ethnicity19), preterm delivery (defined as delivery < 37 weeks), Apgar score < 7 at 5 minutes, and admission to the neonatology department. The presence of neonatal hypoglycaemia was defined as a blood glucose level < 2.6 mmol/l or treatment with a glucose infusion.
Obstetric complications included: instrumental delivery (forceps or vacuum extraction), planned caesarean section and secondary caesarean section.
Statistical analyses
Maternal characteristics are presented according to the GDM treatment regimens. Continuous data are presented as mean with standard deviation or as median and interquartile range [IQR] in case of skewed distribution. Categorical data are presented as number and percentage. For continuous data, the differences between the groups were tested using Student’s unpaired t-test or the Mann-Whitney U test in case of skewed distribution. Categorical variables were compared using the Chi-square test and Fisher’s exact test.
To examine the potential predictors of need for insulin therapy in GDM, analyses were performed using logistic regression models to calculate the odds ratios (ORs) and 95% confidence intervals (95% CIs). Factors considered in the model were: maternal age, smoking during pregnancy, parity, ethnicity, history of PCOS, history of IUFD, pre-gestational BMI, previous GDM, previous neonate weighing ≥ 4500 gram, first-degree relative with diabetes, chronic hypertension, HbA1c, fasting glucose level at time of GDM diagnosis (quartiles), and two-hour glucose level after a 75-gram OGTT at time of GDM diagnosis (quartiles). First univariable logistic regression was performed and significant factors (two-sided p-value < 0.10) were included in a multivariable backward stepwise logistic regression model to determine the final model. In the final prediction model a two-sided p-value < 0.10 was considered statistically significant.
To determine a potential ‘low-risk’ diet-treated group, women with other indications for induction in secondary care – according to the ‘List of Obstetric Indications’ used by midwives in the Netherlands20 – were excluded. The diet group was stratified in a group without and with obstetric and/or neonatal complications as defined above. Comparison between the risk groups was applied using the Mann-Whitney-U test or Chi-square test. Receiver operating characteristics curve analysis was used to evaluate the predicted probability. All p-values were two sided and p < 0.05 was considered statistically significant. All statistical analyses were performed with the use of the statistical package IBM SPSS Statistics (version 22.0. Armonk, NY: IBM Corp).
RESULTS
Maternal characteristics
The most important characteristics of the study population are summarised in table 1. A total of 820 GDM women were referred for treatment, 460 women (56%) were able to maintain adequate glycaemic control with dietary advice only, while 360 (44%) required additional insulin therapy. Of the women who required insulin therapy, 143 women (40%) received trice daily pre-prandial ultrashortacting insulin, 165 women (46%) received basal-bolus insulin therapy, and 39 women (11%) received once daily long-acting insulin (for 13 women the type of insulin was not recorded) at the end of their pregnancy. The median insulin dose was 22 U/day; IQR 12-42 U/day.
The women in the insulin group were older, were more often multiparous, and had a higher pre-gestational BMI. No differences in earlier diagnosis of PCOS, hypertension, history of spontaneous abortion, smoking during pregnancy, and ethnicity were observed between the groups. The frequency rates of previous GDM, a previous neonate weighing ≥ 4500 gram at birth, and first-degree relative with diabetes were higher in the insulin group. The median fasting glucose level and two-hour glucose level after a 75-gram OGTT at time of GDM diagnosis were higher in the insulin-group compared with the diet group. 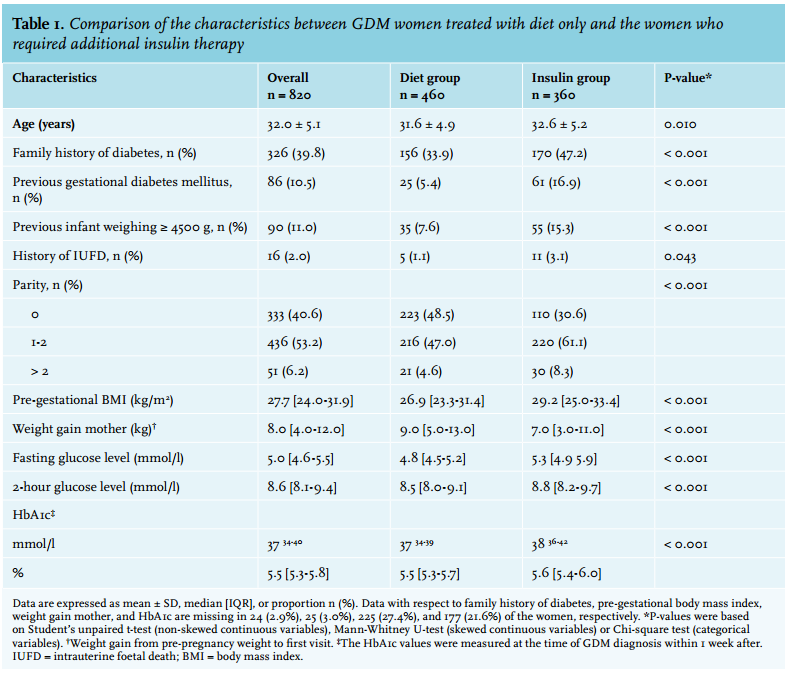
Predictors of need for insulin therapy
Table 2 shows the significant predictors of need for insulin therapy. Previous GDM, family history of diabetes, a previous infant weighing ≥ 4500 gram, Middle-Eastern/ North-African descent, multiparity, pre-gestational BMI ≥ 30 kg/m2 , and an increased fasting glucose level and two-hour glucose after a 75-gram OGTT at GDM diagnosis were significant predictors of need for insulin therapy, with a fasting glucose level ≥ 5.5 mmol/l having the highest OR 6.03; CI 3.56-10.22.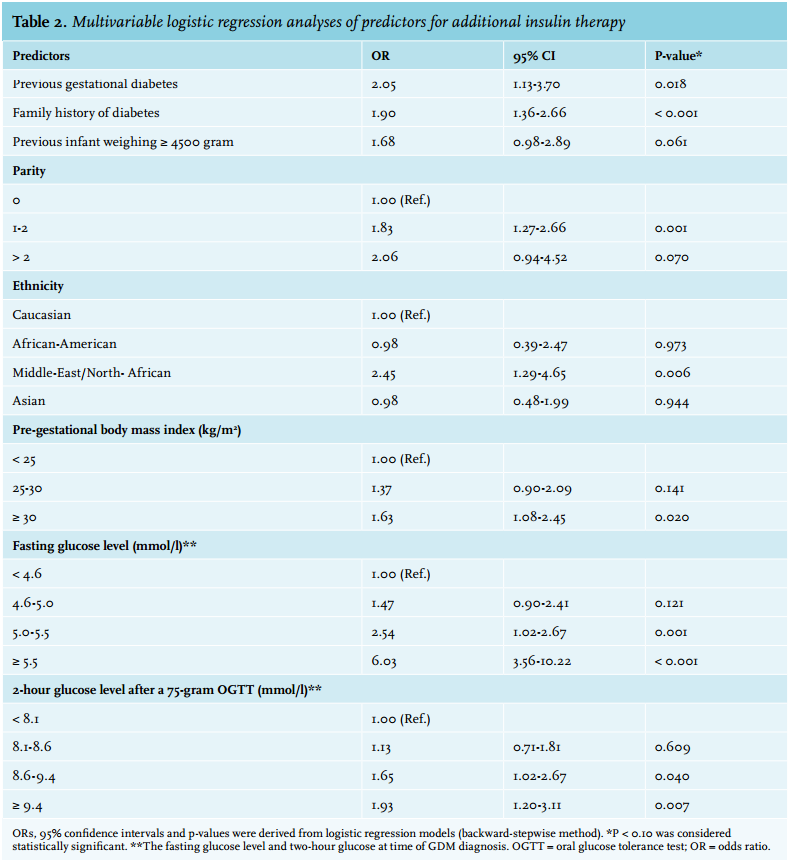
Stratification of diet-treated group
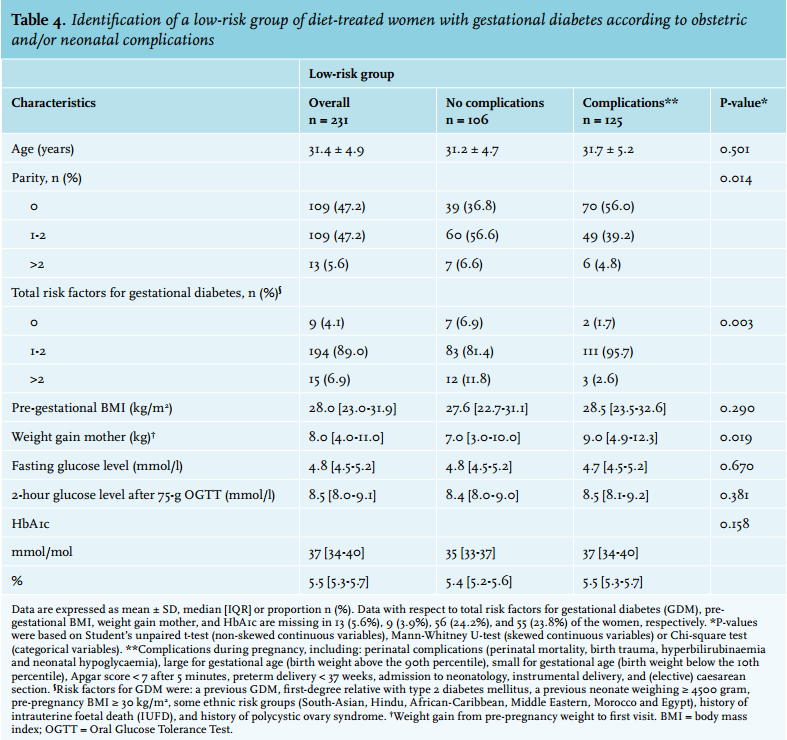
Of the 460 diet-treated women, 229 women (49.8%) were excluded because of other indications for induction. Table 3 gives an overview of these indications. Table 4 shows GDM pregnancies without (106 women (45.9%)) and with (125 women (54.1%)) obstetric and/or neonatal complications. Primiparity and higher weight gain during pregnancy were the best predictors for complications (predictive probability 0.586 and 0.603) respectively.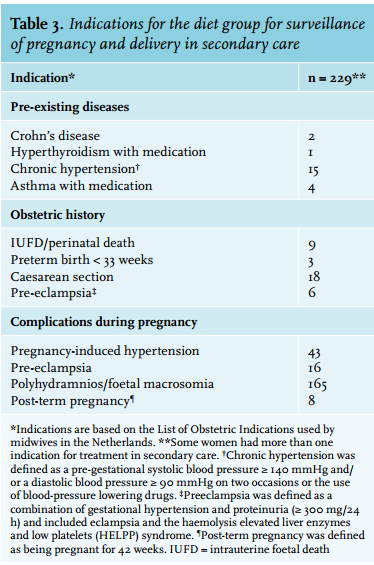
DISCUSSION
In this study we identified the following risk factors in GDM that predicted the need for additional insulin therapy: previous GDM, family history of diabetes, a previous infant weighing ≥ 4500 gram, Middle-Eastern/ North-African descent, multiparity, pre-gestational BMI ≥ 30 kg/m2 , and a markedly increased fasting and two-hour glucose level after a 75-gram OGTT at time of GDM diagnosis. A fasting glucose level ≥ 5.5 mmol/l at time of GDM diagnosis was the strongest predictor of need for insulin therapy.
Moreover, the study showed that diet-treated primiparous women with GDM had more obstetric and/or neonatal complications compared with multiparous women. Also, a higher weight gain in diet-treated women with GDM was associated with more pregnancy complications.
Predictors of need for insulin therapy
Women who receive dietary advice but fail to maintain glycaemic control within 1-2 weeks generally receive additional insulin therapy. In several studies insulin therapy was required in ~20-30% of the women with GDM.12,13,21,22 In our study a higher percentage (44%) of women with GDM required additional insulin therapy. This is in line with two other studies which reported that 51-53% needed insulin therapy.23,24 Possible explanations for the wide range in percentages for insulin need between studies are: differences in the study population, dietary compliance, criteria for diagnosis of GDM, and criteria to start insulin therapy.
A number of previous studies have addressed the possible predictors of the need for insulin therapy in women with GDM. In analogy to our study, three comparable studies with regard to sample size and ethnicity showed that elevated fasting plasma glucose at time of GDM diagnosis was a potent predictor for additional insulin therapy.23-25 One study25 showed in a large cohort of 2365 women with GDM that women requiring insulin therapy were more likely to have a fasting blood glucose of > 5.3 mmol/l (> 95 mg/dl) before a 100-gram OGTT. Moreover, the study found that multiparity, obesity, history of GDM, diagnosis, a three-hour glucose tolerance test > 7.8 mmol/l (> 140 mg/dl), and HbA1c of ≥ 6.0% at GDM diagnosis were additional predictors of the need for insulin therapy. In a second study,23 BMI, gestational age when GDM was diagnosed, and fasting and two-hour glucose levels after a 75-gram OGTT were independent predictors of insulin therapy among 612 women with GDM. For each increase of 0.5 mmol/l to the level of the fasting glucose, they reported an OR for insulin therapy of 2.75. The last study24 identified a number of significant predictors for insulin including measures of glycaemia – fasting glucose level – diagnosis, and family history of GDM among 3009 women with GDM. However, they found a low predictive power for the risk factors.
Although the aforementioned studies used different glucose targets and screening strategies, comparable results regarding fasting glucose levels were observed.
Similar to our study, these studies used ‘old’ diagnostic criteria, before the implementation of the more stringent criteria of the International Association of Diabetes and Pregnancy Study Groups (IADPSG) in 2010.23,24 The fasting glucose level – at time of GDM diagnosis – found in our study (≥ 5.5 mmol/l) is comparable with the national recommended fasting glucose target for start of insulin treatment (≥ 5.3 mmol/l), but much lower than the fasting glucose level used to diagnose GDM (≥ 7.0 mmol/l) according to our current national guideline. The fasting glucose level is more comparable with the new diagnostic criteria adopted by the IADPSG and the WHO 2013 (fasting glucose ≥ 5.1 mmol/l; one-hour ≥ 10.0 mmol/l; and a two-hour value ≥ 8.5 mmol/l).26,27 Revision of the diagnostic criteria of our national guideline seems justified, to overcome the discrepancy between the diagnostic cut-off and treatment target values of fasting glucose in GDM.
The fasting glucose level was a more potent predictor of the need for insulin therapy than the two-hour glucose level at time of the OGTT. The finding that a fasting glucose level is a strong predictor for insulin therapy may be explained by the pathophysiology of GDM and type 2 DM. In GDM, fasting glucose levels may remain normal, when insulin resistance is initially compensated by increased insulin production and therefore the abnormality might only be seen in the postprandial blood glucose values.28 However, it has been demonstrated that GDM women not only have defects in insulin sensitivity but also in insulin secretion.28
Studies also suggest that the fasting glucose level on diagnostic OGTT is more associated with a defect in basal insulin secretion; this might be a plausible explanation why the fasting glucose level is a strong predictor for the need of insulin.29,30 Finally, it has been shown that elevated glucose levels during pregnancy also predict the development of type 2 DM after pregnancy.31 So it may be that women with more pronounced increased fasting plasma glucose are already in an advanced stage to develop type 2 DM.
Stratification of diet-treated group
After the findings on the benefits of GDM treatment, worldwide revisions of the guidelines for screening and diagnosis of GDM were performed.9,12,13 Lowering the diagnostic threshold strongly increases the number of women referred for treatment, which imposes a large burden on obstetric healthcare worldwide due to higher costs.5-7
This study allowed the recognition of a more complex-care group of insulin-treated women with GDM, but on the other hand a potential ‘low-risk’ group of women who can be treated with diet alone, and who could possibly be referred back to primary care. Only primiparity and weight gain during pregnancy were risk factors to develop obstetric and/or neonatal complications in the diet group, but these risk factors had a very low predictive probability. The rather large proportion of 54% of the diet-treated women who suffered pregnancy-related complications could not validly be identified beforehand. Therefore, it is not possible to identify a circumscribed ‘low-risk’ diet-treated group from our data based on pregnancy outcomes. As some authors suggest that diet-treated women – who are likely to maintain good glycaemic control throughout pregnancy with diet only – can be referred back to midwives in primary care,23,32 there remains uncertainty regarding the possible development of pregnancy-related complications. To be able to refer women back to primary care, a healthcare system with optimal interaction and communication between primary and secondary care is required. However, such shared-care models require further evaluation for GDM care. There is more need for prospective studies investigating the safety of treating diet-only women with GDM in primary care.
The strengths of the study are the large cohort of women with GDM and the large database with the collection of commonly used measures. A limitation of the study is the retrospective nature of the analyses and the fact that this GDM cohort is based on the ‘old’ WHO 1999 diagnostic criteria for GDM in our national guideline, which differ greatly from the new WHO 2013 criteria, while for treatment of GDM we use the new stringent international glucose targets in GDM pregnancies. This discrepancy clearly needs reconsideration of the current Dutch guideline on diagnosis and treatment of GDM.
In summary, in this GDM population we found various relevant factors predicting the need for additional insulin therapy in GDM. Especially, a fasting glucose level ≥ 5.5 mmol/l at GDM diagnosis was the strongest predictor of need for insulin therapy. These predictors might be helpful to recognise a complex-care group of insulin-treated women within the GDM population. Women with GDM who had good glycaemic control on diet only with a higher parity and less weight gain, had a lower risk for obstetric and/or neonatal complications. However, from our data a risk-stratification approach for the diet group based on neonatal and obstetric complications alone did not have predictive utility.
ACKNOWLEDGEMENTS
The authors wish to thank the diabetes specialist nurses, and dietitians of the University Medical Center and Martini Hospital Groningen. Further we want to thank: B.J. Schering and M.G. Baas for assistance with the data collection.
DISCLOSURES
Grant support: Novo Nordisk Netherlands provided an unrestricted research grant.
The authors declare no conflicts of interest.
REFERENCES
BIBLIOGRAPHY