KEYWORDS
Zika virus, microcephaly, flavivirus, Aedes, outbreak, Americas
BACKGROUND
In May 2015, the Pan American Health Organization (PAHO) issued an alert about possible autochthonous transmission of Zika virus (ZIKV) in Brazil, South America. Since then, the virus has spread widely in Middle and South America, and the Caribbean, affecting 29 countries and resulting in ten-thousands of probable and confirmed cases as of 22 February 2016.1,2 These include (former) European overseas countries and territories and due to intensive international travel, the risk of importing ZIKV to Europe has increased. On 11 December 2015 the first case of ZIKV imported from the New World was reported in the Netherlands.3 Since then, 30 cases, imported from Suriname and some islands of the (former) overseas territories of the Netherlands, were diagnosed (as of 22 February 2016). Possible association of ZIKV with microcephaly in newborns and other neurological disorders urged the World Health Organization (WHO) to declare the outbreak of microcephaly-associated ZIKV a Public Health Emergency of International Concern on the 1 February.4 Co-circulation of dengue and chikungunya virus, which share overlapping clinical manifestations with ZIKV, complicates clinical diagnosis, while dengue virus, West Nile virus and yellow fever virus may cause cross-reactivity in serological diagnostic tests which severely hampers laboratory diagnosis of ZIKV infection in the outbreak region.5
Here, we briefly provide an overview of the current outbreak, and some characteristics of the virus, clinical manifestations and management of ZIKV infections, and finally the diagnostic tools which can be used.
EPIDEMIOLOGY
ZIKV is a member of the genus Flavivirus, family Flaviviridae. Other flaviviruses of importance to human health are dengue virus, West Nile virus, yellow fever virus, Japanese encephalitis virus and tick-borne encephalitis virus. ZIKV is most closely related to the New World flaviviruses St. Louis encephalitis virus, Rocio virus and Ilheus virus.5,6 ZIKV was first discovered in the Zika forest in Uganda in 1947 and incidental cases were reported for the next 60 years in both Africa and South-East Asia.6 In 2007, ZIKV caused an outbreak of mild disease in the Pacific, characterised by fever, rash, arthralgia and conjunctivitis in Micronesia. This was followed by an epidemic with an estimated 32,000 patients in French Polynesia in 2013-2014.7-9 Since then, the virus has extended its geographic distribution to multiple countries in the Pacific Ocean and ZIKV emerged for the first time in the Americas on Easter Island, Chile in 2014.10 In May 2015, the authorities in Brazil confirmed autochthonous transmission in the northeast of the country and since then, the virus has spread rapidly in the region with ten-thousands of cases (figure 1). In addition, there is a ZIKV outbreak on the Cape Verde islands with approximately 7000 cases recorded since December 2015. The current outbreak in the Americas has led to an increase of travel-associated imported ZIKV cases to Europe with registered cases in Austria, Denmark, Finland, France, Germany, Ireland, Italy, Portugal, the Netherlands, Spain, Sweden, Switzerland and the United Kingdom.2
ZIKV is transmitted in a human-mosquito-human cycle involving Aedes mosquitoes. Ae. aegypti is the only species for which transmission outside Africa has been confirmed. Although competence for Ae. albopictus, a mosquito species established in large parts of Southern Europe and occasionally introduced into the Netherlands by trade of plants and used tires,11 has been demonstrated in laboratory circumstances for the African lineage of ZIKV,12 this mosquito species has never been implied in ZIKV epidemiology outside Africa.6,13,14 Blood transfusion mediated, perinatal and possible sexual transmission of ZIKV have been reported as well.6,15-20 The potential for transmission of ZIKV by other Aedes mosquitos in Europe is under investigation, but is considered to be low.
VIROLOGY
Viruses of the genus flavivirus are positive-stranded, enveloped RNA viruses with a single genome of approximately 11 kb. The ZIKV genome encodes for three structural proteins C, M and E, and seven non-structural proteins, NS1, NS2a, NS2b, NS3, NS4a, NS4b and NS5.6,21 Because the RNA-dependent-RNA-polymerase (NS5) is very conserved among flaviviruses, this genomic region is often used as a target in pan-flavi molecular tests.
ZIKV belongs to the Spondweni serogroup, together with Spondweni virus which circulates in Sub-Saharan Africa and Papua New Guinea. Two lineages of ZIKV are recognised: the African lineage and the Asian lineage.6 The African lineage has not (yet) disseminated outside Africa. ZIKV strains circulating in the Americas are of the Asian lineage with 99.9% identity with the ZIKV strains circulating in French Polynesia in 2013-2014.22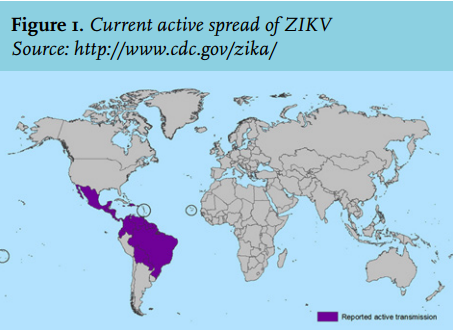
CLINICAL MANIFESTATIONS
Knowledge about the clinical course of ZIKV infection is based on a relatively small number of studies in comparison with other emerging pathogens. The first documented case of human ZIKV infection dates back to 1964 and describes a febrile illness that, without diagnostics proving ZIKV to be the causative agent, could easily have been caused by another arboviral infection, such as dengue or chikungunya.6,9 The majority of ZIKV infections seem to be asymptomatic, confirmed by data from outbreaks in Micronesia and French Polynesia in 2007 and 2013-2014, respectively, with symptoms in only 18% of patients with documented antibodies. However, overestimation of the number of asymptomatic infections may be considered, since serological cross reactivity may have occurred with other circulating flaviviruses such as dengue virus, West Nile virus and Japanese encephalitis virus.23 Other evidence for the occurrence of asymptomatic infections came from studies in blood donors that show a significant seroprevalence.24,25
After an incubation period of 3-12 days, symptomatic patients generally present with fever, arthralgia, myalgia, headache, non-purulent conjunctivitis, and maculopapular rash.26,27 The arthralgia is most often localised in the small joints of hands and feet and could be accompanied with joint swelling.6,7,9 Other manifestations include anorexia, nausea and vomiting, diarrhoea, abdominal pain, sore throat, retro-orbital pain, a burning sensation of the palms and soles and vertigo.6,7,9,28 In contrast to dengue virus infection, haemorrhagic complications seem rarely to be associated with ZIKV, and leukopenia and thrombocytopenia seem to only occur in a minority of ZIKV cases.9,28 Oedema of the extremities, noticed as swelling of especially the ankles, is considered to be quite specific for ZIKV in comparison with dengue and chikungunya virus.9,23 Although not much is known yet about the morbidity and mortality of the current ZIKV outbreak, it is assumed that in comparison with other arboviral infections, ZIKV is relatively mild and self-limiting. Currently, three deaths have been linked to ZIKV infection, although, the level of evidence for causality remains doubtful.9,23 In the current ZIKV outbreak, much attention has been drawn towards potential neurological complications of ZIKV infection, where the main concerns are the possible association of ZIKV infection with Guillain-Barré syndrome (GBS) and microcephaly as a neurological manifestations in newborns.29-31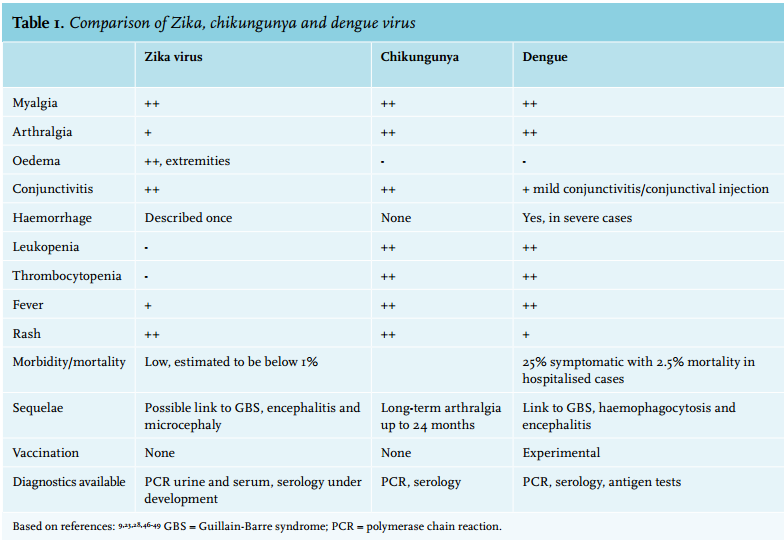
Both complications were observed in the outbreak in French Polynesia29 as well as in the current outbreak, with Brazil reporting more than 4700 suspected cases of microcephaly since May 2015. One should bear in mind that only a minority of these 4700 cases remained linked to ZIKV infection after correction for differing criteria for microcephaly, birth weight and potential other factors predisposing to microcephaly. ZIKV RNA was identified in the amniotic fluid of two women whose foetuses had microcephaly.30 The potential causality is further supported by the full genome detection of the virus in the brain of a foetus with microcephaly.31 Several countries reported spikes in GBS cases in January 2016.28-30,32,33 Recently, a confirmed imported ZIKV case developed GBS in the Netherlands (van den Beukel et al. submitted). The causality between ZIKV infection and GBS is not yet proven and a possible mechanism can only be hypothesised. Hypothetically, a possible underlying mechanism could be similar to that of Campylobacter-driven GBS, involving molecular mimicry where antibodies against the pathogen cross react with antigens on nerve tissue and thereby damage healthy nerves.34 Alternatively, the GBS-like symptoms may be caused by direct virus-induced nerve damage.
While evidence supports the potential for foetal infection with ZIKV, much remains unknown about the strength of this association, and – if confirmed – the prevalence of intra-uterine infections and subsequent complications in ZIKV-infected pregnant women. Similar to other infections during pregnancy, it is likely that effects – should they occur – differ depending on the timing of the infection, potentially ranging from miscarriage, to birth defects, to the birth of apparently healthy babies with or without some more subtle sequellae. Studies have shown that physiological skewing of the immune system during pregnancy to a more immune tolerant state may lead to delayed clearance of infection, and thus prolonged viraemia and increased risk of foetal infection. Of course, all this assumes a combination with a potential neurotropism for ZIKV which has not yet been proven in animal models. Furthermore, it remains to be seen whether specific ZIKV strains have changed in virulence or whether possible complications such as GBS and microcephaly were unnoticed in the past due to their relatively low absolute numbers. Additional studies, both epidemiological and animal models, are needed to establish the possible association between ZIKV infection and these complications.
CLINICAL MANAGEMENT AND TREATMENT
No specific antiviral treatment is available thus, if needed, care is supportive. However, the disease is self-limiting and mainly lasts no longer than seven days in the majority of cases. Since there is no evidence yet for haemorrhagic complications in ZIKV, the use of non-steroidal anti-inflammatory drugs (NSAIDs) in case of (severe) arthralgia is not strictly contraindicated.28 However, in case of uncertainty of the diagnosis and the possibility of a dengue virus infection pending the test results, NSAIDs should still be avoided. In daily practice, normal thrombocyte counts could favour the use of NSAIDs.28 Where possible acetaminophen, which does not alter platelet aggregation, could be used to supress milder symptoms.
In case of GBS, intravenous immunoglobulin might be effective, although severe GBS cases may require intensive care, including mechanical ventilation.29,35 Currently, the Centers for Disease Control (CDC) recommends monitoring of foetal development in pregnant women with evidence of ZIKV infection by 3-4 weekly ultrasounds. This strategy would increase the knowledge about causality of ZIKV-infected pregnant women and birth defects. However, the benefits for the mother and unborn child are limited due to the lack of treatment or intervention other than abortion.35,36 Currently, the Dutch National Institute for Public Health and the Environment (RIVM), advises pregnant women, when possible, to postpone non-essential travel to ZIKV outbreak areas. If travel is necessary, mosquito repellents, long sleeved clothing and an impregnated bed net should be used. When a pregnant woman has a molecular proven ZIKV infection, follow-up in a specialised perinatal care centre during the pregnancy is recommended (http://www.rivm.nl/dsresource?objectid =rivmp:304780&type=org&disposition=inline&ns_nc=1).
DIFFERENTIAL DIAGNOSIS
Since the majority of symptomatic ZIKV patients present with arthralgia, fever and rash, the differential diagnosis of suspected ZIKV includes viruses with similar clinical manifestations, like chikungunya and dengue virus.6,37 Based on the geographical exposure, the differential diagnosis can be broadened. For the Americas the alphaviruses Mayaro virus, Oropouche virus and equine encephalitis virus, as well as West Nile virus and La Crosse encephalitis virus may be considered. Also, malaria and rickettsioses may be taken into account.28,38 The differential diagnosis can be broadened to other acute virus infections including influenza, rubella and measles, or non-viral diseases.
DIAGNOSTICS
Information on ZIKV infection kinetics is indispensable for proper interpretation of diagnostic results. The information available in literature is limited to Asian ZIKV and concerns only a few cases.39 Viraemia seems low and short. ZIKV shows a peak in viral load when symptoms appear and can be detected up to 3-5 days after onset of symptoms with reverse transcription polymerase chain reaction (RT-PCR).32,40,41 ZIKV RNA has been detected in saliva, nasopharyngeal swabs, urine and semen as well.17,20,42-44 A combination of blood, urine and saliva samples is advised to increase both the sensitivity of molecular detection and the detection window. The viral load in urine seems to be higher than in blood/serum, is observed to peak 5-7 days upon onset of symptoms and has a much longer detection window (detection > 28 days post-onset of symptoms have been described) than blood, although sensitivity of detection at these time points remains to be determined.39 A combination of blood and saliva sampling increased the ZIKV detection rate by 19% but did not increase the detection window.17 ZIKV specific IgM seems to appear 3-5 days and IgG 10 days after onset of illness in patients without previous flavivirus infections. Typically in flavivirus infections IgM develops within a few days upon onset of symptoms and is generally detectable up to three months. IgG develops a few days later and is typically detectable for months to years.5,32 More studies are needed to validate these observations.
Multiple real-time and conventional RT-PCRs specific for ZIKV or pan-flavi, and serology tests have been described in the literature or are commercially available.39 All still need extensive validation in the context of both the outbreak region and areas were cases are imported. Patients in the current outbreak region will have a high level flavivirus background while travellers returning to Europe will generally have been exposed to these viruses to a far lesser extent. This is especially important for serology-based testing as extensive cross-reactivity between antibodies triggered by different flavivirus infections or vaccination exist. Furthermore, an acute ZIKV infection might boost cross-reactive antibodies due to prior flavivirus infection/vaccination. This will complicate diagnosis based on serology in the outbreak region and will require detailed knowledge on the vaccination history for Japanese encephalitis virus, tick-borne encephalitis virus and yellow fever virus when interpreting diagnostic results of returning travellers.5,39,45 The availability of discriminating ZIKV serology is especially important to identify asymptomatic ZIKV infections in pregnant women due to putative teratogenic effects.
CONCLUDING REMARKS
The current outbreak of ZIKV in the Americas, including Dutch (former) overseas territories, has direct implications for infectious disease specialists, obstetricians, midwifes and microbiologists in the Netherlands. Besides dengue and chikungunya virus, clinicians should also include ZIKV in their differential diagnosis of fever with rash in travellers returning from Asia, Africa, the Pacific ocean area and the Americas. Although ZIKV infections usually manifest as asymptomatic or mild, infection of women during pregnancy requires intensive follow-up due to putative correlation with neurological defects in newborns, until the link between ZIKV and microcephaly has been substantiated or rejected. Determination of asymptomatic ZIKV infection during pregnancy is complicated due to extensive cross-reactivity in serology-based testing. For diagnosis in acutely infected patients a combination of blood, urine and saliva will increase the sensitivity and window of ZIKV detection. Current ongoing international collaborative studies might give insight in these issues on short notice.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES